Alzheimer's disease (AD), also known in medical literature as Alzheimer disease, is the most common form of dementia. There is no cure for the disease, which worsens as it progresses, and eventually leads to death. It was first described by German psychiatrist and neuropathologist Alois Alzheimer in 1906 and was named after him.[1]
Most often, AD is diagnosed in people over 65 years of age,[2] although the less-prevalent early-onset Alzheimer's can occur much earlier. In 2006, there were 26.6 million sufferers worldwide. Alzheimer's is predicted to affect 1 in 85 people globally by 2050.[3]
Although Alzheimer's disease develops differently for every individual, there are many common symptoms.[4] Early symptoms are often mistakenly thought to be 'age-related' concerns, or manifestations of stress.[5] In the early stages, the most common symptom is difficulty in remembering recent events. When AD is suspected, the diagnosis is usually confirmed with tests that evaluate behaviour and thinking abilities, often followed by a brain scan if available.[6]
As the disease advances, symptoms can include confusion, irritability and aggression, mood swings, trouble with language, and long-term memory loss. As the sufferer declines they often withdraw from family and society.[5][7] Gradually, bodily functions are lost, ultimately leading to death.[8] Since the disease is different for each individual, predicting how it will affect the person is difficult. AD develops for an unknown and variable amount of time before becoming fully apparent, and it can progress undiagnosed for years. On average, the life expectancy following diagnosis is approximately seven years.[9] Fewer than three percent of individuals live more than fourteen years after diagnosis.[10]
The cause and progression of Alzheimer's disease are not well understood. Research indicates that the disease is associated with plaques and tangles in the brain.[11] Current treatments only help with the symptoms of the disease. There are no available treatments that stop or reverse the progression of the disease. As of 2012[update], more than 1000 clinical trials have been or are being conducted to find ways to treat the disease, but it is unknown if any of the tested treatments will work.[12] Mental stimulation, exercise, and a balanced diet have been suggested as ways to delay symptoms in healthy older individuals, but there is no conclusive evidence supporting an effect.[13]
Because AD cannot be cured and is degenerative, the sufferer relies on others for assistance. The role of the main caregiver is often taken by the spouse or a close relative.[14] Alzheimer's disease is known for placing a great burden on caregivers; the pressures can be wide-ranging, involving social, psychological, physical, and economic elements of the caregiver's life.[15][16][17] In developed countries, AD is one of the most costly diseases to society.[18][19]
The disease course is divided into four stages, with progressive patterns of cognitive and functional impairments.
The first symptoms are often mistakenly attributed to ageing or stress.[5] Detailed neuropsychological testing can reveal mild cognitive difficulties up to eight years before a person fulfils the clinical criteria for diagnosis of AD.[20] These early symptoms can affect the most complex daily living activities.[21] The most noticeable deficit is memory loss, which shows up as difficulty in remembering recently learned facts and inability to acquire new information.[20][22]
Subtle problems with the executive functions of attentiveness, planning, flexibility, and abstract thinking, or impairments in semantic memory (memory of meanings, and concept relationships) can also be symptomatic of the early stages of AD.[20] Apathy can be observed at this stage, and remains the most persistent neuropsychiatric symptom throughout the course of the disease.[23] The preclinical stage of the disease has also been termed mild cognitive impairment,[22] but whether this term corresponds to a different diagnostic stage or identifies the first step of AD is a matter of dispute.[24]
In people with AD the increasing impairment of learning and memory eventually leads to a definitive diagnosis. In a small portion of them, difficulties with language, executive functions, perception (agnosia), or execution of movements (apraxia) are more prominent than memory problems.[25] AD does not affect all memory capacities equally. Older memories of the person's life (episodic memory), facts learned (semantic memory), and implicit memory (the memory of the body on how to do things, such as using a fork to eat) are affected to a lesser degree than new facts or memories.[26][27]
Language problems are mainly characterised by a shrinking vocabulary and decreased word fluency, which lead to a general impoverishment of oral and written language.[25][28] In this stage, the person with Alzheimer's is usually capable of adequately communicating basic ideas.[25][28][29] While performing fine motor tasks such as writing, drawing or dressing, certain movement coordination and planning difficulties (apraxia) may be present but they are commonly unnoticed.[25] As the disease progresses, people with AD can often continue to perform many tasks independently, but may need assistance or supervision with the most cognitively demanding activities.[25]
Progressive deterioration eventually hinders independence; with subjects being unable to perform most common activities of daily living.[25] Speech difficulties become evident due to an inability to recall vocabulary, which leads to frequent incorrect word substitutions (paraphasias). Reading and writing skills are also progressively lost.[25][29] Complex motor sequences become less coordinated as time passes and AD progresses, so the risk of falling increases.[25] During this phase, memory problems worsen, and the person may fail to recognise close relatives.[25] Long-term memory, which was previously intact, becomes impaired.[25]
Behavioural and neuropsychiatric changes become more prevalent. Common manifestations are wandering, irritability and labile affect, leading to crying, outbursts of unpremeditated aggression, or resistance to caregiving.[25] Sundowning can also appear.[30] Approximately 30% of people with AD develop illusionary misidentifications and other delusional symptoms.[25] Subjects also lose insight of their disease process and limitations (anosognosia).[25] Urinary incontinence can develop.[25] These symptoms create stress for relatives and caretakers, which can be reduced by moving the person from home care to other long-term care facilities.[25][31]
During the final stage of AD, the person is completely dependent upon caregivers.[25] Language is reduced to simple phrases or even single words, eventually leading to complete loss of speech.[25][29] Despite the loss of verbal language abilities, people can often understand and return emotional signals.[25] Although aggressiveness can still be present, extreme apathy and exhaustion are much more common results.[25] People with AD will ultimately not be able to perform even the simplest tasks without assistance.[25] Muscle mass and mobility deteriorate to the point where they are bedridden, and they lose the ability to feed themselves.[25] AD is a terminal illness, with the cause of death typically being an external factor, such as infection of pressure ulcers or pneumonia, not the disease itself.[25]

Microscopy image of a neurofibrillary tangle, conformed by hyperphosphorylated
tau protein
The cause for most Alzheimer's cases is still essentially unknown[32][33] (except for 1% to 5% of cases where genetic differences have been identified). Several competing hypotheses exist trying to explain the cause of the disease. The oldest, on which most currently available drug therapies are based, is the cholinergic hypothesis,[34] which proposes that AD is caused by reduced synthesis of the neurotransmitter acetylcholine. The cholinergic hypothesis has not maintained widespread support, largely because medications intended to treat acetylcholine deficiency have not been very effective. Other cholinergic effects have also been proposed, for example, initiation of large-scale aggregation of amyloid,[35] leading to generalised neuroinflammation.[36]
In 1991, the amyloid hypothesis postulated that amyloid beta (Aβ) deposits are the fundamental cause of the disease.[37][38] Support for this postulate comes from the location of the gene for the amyloid beta precursor protein (APP) on chromosome 21, together with the fact that people with trisomy 21 (Down Syndrome) who have an extra gene copy almost universally exhibit AD by 40 years of age.[39][40] Also APOE4, the major genetic risk factor for AD, leads to excess amyloid buildup in the brain.[41] Further evidence comes from the finding that transgenic mice that express a mutant form of the human APP gene develop fibrillar amyloid plaques and Alzheimer's-like brain pathology with spatial learning deficits.[42]
An experimental vaccine was found to clear the amyloid plaques in early human trials, but it did not have any significant effect on dementia.[43] Researchers have been led to suspect non-plaque Aβ oligomers (aggregates of many monomers) as the primary pathogenic form of Aβ. These toxic oligomers, also referred to as amyloid-derived diffusible ligands (ADDLs), bind to a surface receptor on neurons and change the structure of the synapse, thereby disrupting neuronal communication.[44] One receptor for Aβ oligomers may be the prion protein, the same protein that has been linked to mad cow disease and the related human condition, Creutzfeldt-Jakob disease, thus potentially linking the underlying mechanism of these neurodegenerative disorders with that of Alzheimer's disease.[45]
In 2009, this theory was updated, suggesting that a close relative of the beta-amyloid protein, and not necessarily the beta-amyloid itself, may be a major culprit in the disease. The theory holds that an amyloid-related mechanism that prunes neuronal connections in the brain in the fast-growth phase of early life may be triggered by ageing-related processes in later life to cause the neuronal withering of Alzheimer's disease.[46] N-APP, a fragment of APP from the peptide's N-terminus, is adjacent to beta-amyloid and is cleaved from APP by one of the same enzymes. N-APP triggers the self-destruct pathway by binding to a neuronal receptor called death receptor 6 (DR6, also known as TNFRSF21).[46] DR6 is highly expressed in the human brain regions most affected by Alzheimer's, so it is possible that the N-APP/DR6 pathway might be hijacked in the ageing brain to cause damage. In this model, beta-amyloid plays a complementary role, by depressing synaptic function.
A 2004 study found that deposition of amyloid plaques does not correlate well with neuron loss.[47] This observation supports the tau hypothesis, the idea that tau protein abnormalities initiate the disease cascade.[38] In this model, hyperphosphorylated tau begins to pair with other threads of tau. Eventually, they form neurofibrillary tangles inside nerve cell bodies.[48] When this occurs, the microtubules disintegrate, collapsing the neuron's transport system.[49] This may result first in malfunctions in biochemical communication between neurons and later in the death of the cells.[50]
Herpes simplex virus type 1 has also been proposed to play a causative role in people carrying the susceptible versions of the apoE gene.[51]
Another hypothesis asserts that the disease may be caused by age-related myelin breakdown in the brain. Iron released during myelin breakdown is hypothesised to cause further damage. Homeostatic myelin repair processes contribute to the development of proteinaceous deposits such as amyloid-beta and tau.[52][53][54]
Oxidative stress and dys-homeostasis of biometal (biology) metabolism may be significant in the formation of the pathology.[55][56]
AD individuals show 70% loss of locus coeruleus cells that provide norepinephrine (in addition to its neurotransmitter role) that locally diffuses from "varicosities" as an endogenous antiinflammatory agent in the microenvironment around the neurons, glial cells, and blood vessels in the neocortex and hippocampus.[57] It has been shown that norepinephrine stimulates mouse microglia to suppress Aβ-induced production of cytokines and their phagocytosis of Aβ.[57] This suggests that degeneration of the locus ceruleus might be responsible for increased Aβ deposition in AD brains.[57]

Histopathologic image of senile plaques seen in the cerebral cortex of a person with Alzheimer's disease of presenile onset. Silver impregnation.
Alzheimer's disease is characterised by loss of neurons and synapses in the cerebral cortex and certain subcortical regions. This loss results in gross atrophy of the affected regions, including degeneration in the temporal lobe and parietal lobe, and parts of the frontal cortex and cingulate gyrus.[36] Studies using MRI and PET have documented reductions in the size of specific brain regions in people with AD as they progressed from mild cognitive impairment to Alzheimer's disease, and in comparison with similar images from healthy older adults.[58][59]
Both amyloid plaques and neurofibrillary tangles are clearly visible by microscopy in brains of those afflicted by AD.[11] Plaques are dense, mostly insoluble deposits of amyloid-beta peptide and cellular material outside and around neurons. Tangles (neurofibrillary tangles) are aggregates of the microtubule-associated protein tau which has become hyperphosphorylated and accumulate inside the cells themselves. Although many older individuals develop some plaques and tangles as a consequence of ageing, the brains of people with AD have a greater number of them in specific brain regions such as the temporal lobe.[60] Lewy bodies are not rare in the brains of people with AD.[61]

Enzymes act on the APP (amyloid precursor protein) and cut it into fragments. The beta-amyloid fragment is crucial in the formation of senile plaques in AD.
Alzheimer's disease has been identified as a protein misfolding disease (proteopathy), caused by accumulation of abnormally folded A-beta and tau proteins in the brain.[62] Plaques are made up of small peptides, 39–43 amino acids in length, called beta-amyloid (also written as A-beta or Aβ). Beta-amyloid is a fragment from a larger protein called amyloid precursor protein (APP), a transmembrane protein that penetrates through the neuron's membrane. APP is critical to neuron growth, survival and post-injury repair.[63][64] In Alzheimer's disease, an unknown process causes APP to be divided into smaller fragments by enzymes through proteolysis.[65] One of these fragments gives rise to fibrils of beta-amyloid, which form clumps that deposit outside neurons in dense formations known as senile plaques.[11][66]

In Alzheimer's disease, changes in tau protein lead to the disintegration of microtubules in brain cells.
AD is also considered a tauopathy due to abnormal aggregation of the tau protein. Every neuron has a cytoskeleton, an internal support structure partly made up of structures called microtubules. These microtubules act like tracks, guiding nutrients and molecules from the body of the cell to the ends of the axon and back. A protein called tau stabilises the microtubules when phosphorylated, and is therefore called a microtubule-associated protein. In AD, tau undergoes chemical changes, becoming hyperphosphorylated; it then begins to pair with other threads, creating neurofibrillary tangles and disintegrating the neuron's transport system.[67]
Exactly how disturbances of production and aggregation of the beta amyloid peptide gives rise to the pathology of AD is not known.[68] The amyloid hypothesis traditionally points to the accumulation of beta amyloid peptides as the central event triggering neuron degeneration. Accumulation of aggregated amyloid fibrils, which are believed to be the toxic form of the protein responsible for disrupting the cell's calcium ion homeostasis, induces programmed cell death (apoptosis).[69] It is also known that Aβ selectively builds up in the mitochondria in the cells of Alzheimer's-affected brains, and it also inhibits certain enzyme functions and the utilisation of glucose by neurons.[70]
Various inflammatory processes and cytokines may also have a role in the pathology of Alzheimer's disease. Inflammation is a general marker of tissue damage in any disease, and may be either secondary to tissue damage in AD or a marker of an immunological response.[71]
Alterations in the distribution of different neurotrophic factors and in the expression of their receptors such as the brain derived neurotrophic factor (BDNF) have been described in AD.[72][73]
The vast majority of cases of Alzheimer's disease are sporadic, meaning that they are not genetically inherited although some genes may act as risk factors. On the other hand, around 0.1% of the cases are familial forms of autosomal dominant (not sex-linked) inheritance, which usually have an onset before age 65.[74] This form of the disease is known as Early onset familial Alzheimer's disease.
Most of autosomal dominant familial AD can be attributed to mutations in one of three genes: amyloid precursor protein (APP) and presenilins 1 and 2.[75] Most mutations in the APP and presenilin genes increase the production of a small protein called Aβ42, which is the main component of senile plaques.[76] Some of the mutations merely alter the ratio between Aβ42 and the other major forms—e.g., Aβ40—without increasing Aβ42 levels.[76][77] This suggests that presenilin mutations can cause disease even if they lower the total amount of Aβ produced and may point to other roles of presenilin or a role for alterations in the function of APP and/or its fragments other than Aβ.
Most cases of Alzheimer's disease do not exhibit autosomal-dominant inheritance and are termed sporadic AD. Nevertheless genetic differences may act as risk factors. The best known genetic risk factor is the inheritance of the ε4 allele of the apolipoprotein E (APOE).[78][79] Between 40 and 80% of people with AD possess at least one APOEε4 allele.[79] The APOEε4 allele increases the risk of the disease by three times in heterozygotes and by 15 times in homozygotes.[74] However, it must be noted that this "genetic" effect is not necessarily purely genetic. For example, certain Nigerian populations have no relationship between presence or dose of APOEε4 and incidence or age-of-onset for Alzheimer's disease.[80] [81] Geneticists agree that numerous other genes also act as risk factors or have protective effects that influence the development of late onset Alzheimer's disease,[75] but results such as the Nigerian studies and the incomplete penetrance for all genetic risk factors associated with sporadic Alzheimers indicate a strong role for environmental effects. Over 400 genes have been tested for association with late-onset sporadic AD,[75] most with null results.[74]

PET scan of the brain of a person with AD showing a loss of function in the temporal lobe
Alzheimer's disease is usually diagnosed clinically from the patient history, collateral history from relatives, and clinical observations, based on the presence of characteristic neurological and neuropsychological features and the absence of alternative conditions.[82][83] Advanced medical imaging with computed tomography (CT) or magnetic resonance imaging (MRI), and with single photon emission computed tomography (SPECT) or positron emission tomography (PET) can be used to help exclude other cerebral pathology or subtypes of dementia.[84] Moreover, it may predict conversion from prodromal stages (mild cognitive impairment) to Alzheimer's disease.[85]
Assessment of intellectual functioning including memory testing can further characterise the state of the disease.[5] Medical organisations have created diagnostic criteria to ease and standardise the diagnostic process for practicing physicians. The diagnosis can be confirmed with very high accuracy post-mortem when brain material is available and can be examined histologically.[86]
The National Institute of Neurological and Communicative Disorders and Stroke (NINCDS) and the Alzheimer's Disease and Related Disorders Association (ADRDA, now known as the Alzheimer's Association) established the most commonly used NINCDS-ADRDA Alzheimer's Criteria for diagnosis in 1984,[86] extensively updated in 2007.[87] These criteria require that the presence of cognitive impairment, and a suspected dementia syndrome, be confirmed by neuropsychological testing for a clinical diagnosis of possible or probable AD. A histopathologic confirmation including a microscopic examination of brain tissue is required for a definitive diagnosis. Good statistical reliability and validity have been shown between the diagnostic criteria and definitive histopathological confirmation.[88] Eight cognitive domains are most commonly impaired in AD—memory, language, perceptual skills, attention, constructive abilities, orientation, problem solving and functional abilities. These domains are equivalent to the NINCDS-ADRDA Alzheimer's Criteria as listed in the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) published by the American Psychiatric Association.[89][90]

Neuropsychological
screening tests can help in the diagnosis of AD. In the tests, people are instructed to copy drawings similar to the one shown in the picture, remember words, read, and subtract serial numbers.
Neuropsychological tests such as the mini-mental state examination (MMSE), are widely used to evaluate the cognitive impairments needed for diagnosis. More comprehensive test arrays are necessary for high reliability of results, particularly in the earliest stages of the disease.[91][92] Neurological examination in early AD will usually provide normal results, except for obvious cognitive impairment, which may not differ from that resulting from other diseases processes, including other causes of dementia.
Further neurological examinations are crucial in the differential diagnosis of AD and other diseases.[5] Interviews with family members are also utilised in the assessment of the disease. Caregivers can supply important information on the daily living abilities, as well as on the decrease, over time, of the person's mental function.[85] A caregiver's viewpoint is particularly important, since a person with AD is commonly unaware of his own deficits.[93] Many times, families also have difficulties in the detection of initial dementia symptoms and may not communicate accurate information to a physician.[94]
Another recent objective marker of the disease is the analysis of cerebrospinal fluid for amyloid beta or tau proteins,[95] both total tau protein and phosphorylated tau181P protein concentrations.[96] Searching for these proteins using a spinal tap can predict the onset of Alzheimer's with a sensitivity of between 94% and 100%.[96] When used in conjunction with existing neuroimaging techniques, doctors can identify people with significant memory loss who are already developing the disease.[96] Spinal fluid tests are commercially available, unlike the latest neuroimaging technology.[97] Alzheimer's was diagnosed in one-third of the people who did not have any symptoms in a 2010 study, meaning that disease progression occurs well before symptoms occur.[98]
Supplemental testing provides extra information on some features of the disease or is used to rule out other diagnoses. Blood tests can identify other causes for dementia than AD[5]—causes which may, in rare cases, be reversible.[99] It is common to perform thyroid function tests, assess B12, rule out syphilis, rule out metabolic problems (including tests for kidney function, electrolyte levels and for diabetes), assess levels of heavy metals (e.g. lead, mercury) and anaemia. (See differential diagnosis for Dementia). (It is also necessary to rule out delirium).
Psychological tests for depression are employed, since depression can either be concurrent with AD (see Depression of Alzheimer disease), an early sign of cognitive impairment,[100] or even the cause.[101][102]
When available as a diagnostic tool, single photon emission computed tomography (SPECT) and positron emission tomography (PET) neuroimaging are used to confirm a diagnosis of Alzheimer's in conjunction with evaluations involving mental status examination.[103] In a person already having dementia, SPECT appears to be superior in differentiating Alzheimer's disease from other possible causes, compared with the usual attempts employing mental testing and medical history analysis.[104] Advances have led to the proposal of new diagnostic criteria.[5][87]
A new technique known as PiB PET has been developed for directly and clearly imaging beta-amyloid deposits in vivo using a tracer that binds selectively to the A-beta deposits.[105] The PiB-PET compound uses carbon-11 PET scanning. Recent studies suggest that PiB-PET is 86% accurate in predicting which people with mild cognitive impairment will develop Alzheimer's disease within two years, and 92% accurate in ruling out the likelihood of developing Alzheimer's.[106]
A similar PET scanning radiopharmaceutical compound called (E)-4-(2-(6-(2-(2-(2-([18F]-fluoroethoxy)ethoxy)ethoxy)pyridin-3-yl)vinyl)-N-methyl benzenamine, or 18F AV-45, or florbetapir-fluorine-18, or simply florbetapir, contains the longer-lasting radionuclide fluorine-18, has recently been created, and tested as a possible diagnostic tool in Alzheimer's disease.[107][108][109][110] Florbetapir, like PiB, binds to beta-amyloid, but due to its use of fluorine-18 has a half-life of 110 minutes, in contrast to PiB's radioactive half life of 20 minutes. Wong et al. found that the longer life allowed the tracer to accumulate significantly more in the brains of people with AD, particularly in the regions known to be associated with beta-amyloid deposits.[110]
One review predicted that amyloid imaging is likely to be used in conjunction with other markers rather than as an alternative.[111]
Volumetric MRI can detect changes in the size of brain regions. Measuring those regions that atrophy during the progress of Alzheimer's disease is showing promise as a diagnostic indicator. It may prove less expensive than other imaging methods currently under study.[112]
Recent studies have shown that people with AD had decreased glutamate (Glu) as well as decreased Glu/creatine (Cr), Glu/myo-inositol (mI), Glu/N-acetylaspartate (NAA), and NAA/Cr ratios compared to normal people. Both decreased NAA/Cr and decreased hippocampal glutamate may be an early indicator of AD.[113]
Early research in mouse models may have identified markers for AD. The applicability of these markers is unknown.[114]
A small human study in 2011 found that monitoring blood dehydroepiandrosterone (DHEA) variations in response to an oxidative stress could be a useful proxy test: the subjects with MCI did not have a DHEA variation, while the healthy controls did.[115]

Intellectual activities such as playing
chess or regular social interaction have been linked to a reduced risk of AD in epidemiological studies, although no causal relationship has been found.
At present, there is no definitive evidence to support that any particular measure is effective in preventing AD.[116] Global studies of measures to prevent or delay the onset of AD have often produced inconsistent results. However, epidemiological studies have proposed relationships between certain modifiable factors, such as diet, cardiovascular risk, pharmaceutical products, or intellectual activities among others, and a population's likelihood of developing AD. Only further research, including clinical trials, will reveal whether these factors can help to prevent AD.[117]
Although cardiovascular risk factors, such as hypercholesterolaemia, hypertension, diabetes, and smoking, are associated with a higher risk of onset and course of AD,[118][119] statins, which are cholesterol lowering drugs, have not been effective in preventing or improving the course of the disease.[120][121] The components of a Mediterranean diet, which include fruit and vegetables, bread, wheat and other cereals, olive oil, fish, and red wine, may all individually or together reduce the risk and course of Alzheimer's disease.[122] The diet's beneficial cardiovascular effect has been proposed as the mechanism of action.[122] There is limited evidence that light to moderate use of alcohol, particularly red wine, is associated with lower risk of AD.[123]
Reviews on the use of vitamins have not found enough evidence of efficacy to recommend vitamin C,[124] E,[124][125] or folic acid with or without vitamin B12,[126] as preventive or treatment agents in AD. Additionally vitamin E is associated with important health risks.[124] Trials examining folic acid (B9) and other B vitamins failed to show any significant association with cognitive decline.[127] Docosahexaenoic acid, an Omega 3 fatty acid, has not been found to slow decline.[128]
Long-term usage of non-steroidal anti-inflammatory drug (NSAIDs) is associated with a reduced likelihood of developing AD.[129] Human postmortem studies, in animal models, or in vitro investigations also support the notion that NSAIDs can reduce inflammation related to amyloid plaques.[129] However trials investigating their use as palliative treatment have failed to show positive results while no prevention trial has been completed.[129] Curcumin from the curry spice turmeric has shown some effectiveness in preventing brain damage in mouse models due to its anti-inflammatory properties.[130][131] Hormone replacement therapy, although previously used, is no longer thought to prevent dementia and in some cases may even be related to it.[132][133] There is inconsistent and unconvincing evidence that ginkgo has any positive effect on cognitive impairment and dementia,[134] and a recent study concludes that it has no effect in reducing the rate of AD incidence.[135] A 21-year study found that coffee drinkers of 3–5 cups per day at midlife had a 65% reduction in risk of dementia in late-life.[136]
People who engage in intellectual activities such as reading, playing board games, completing crossword puzzles, playing musical instruments, or regular social interaction show a reduced risk for Alzheimer's disease.[137] This is compatible with the cognitive reserve theory, which states that some life experiences result in more efficient neural functioning providing the individual a cognitive reserve that delays the onset of dementia manifestations.[137] Education delays the onset of AD syndrome, but is not related to earlier death after diagnosis.[138] Learning a second language even later in life seems to delay getting Alzheimer disease.[139] Physical activity is also associated with a reduced risk of AD.[138]
Two studies have shown that medical marijuana may be effective in inhibiting the progress of AD. The active ingredient in marijuana, THC, may prevent the formation of deposits in the brain associated with Alzheimer's disease. THC was found to inhibit acetylcholinesterase more effectively than commercially marketed drugs.[140][141] A recent review of the clinical research has found no evidence that cannabinoids are effective in the improvement of disturbed behaviour or in the treatment of other symptoms of AD or dementia.[142]
Some studies have shown an increased risk of developing AD with environmental factors such the intake of metals, particularly aluminium,[143][144] or exposure to solvents.[145] The quality of some of these studies has been criticised,[146] and other studies have concluded that there is no relationship between these environmental factors and the development of AD.[147][148][149][150]
While some studies suggest that extremely low frequency electromagnetic fields may increase the risk for Alzheimer's disease, reviewers found that further epidemiological and laboratory investigations of this hypothesis are needed.[151] Smoking is a significant AD risk factor.[152] Systemic markers of the innate immune system are risk factors for late-onset AD.[153]
There is no cure for Alzheimer's disease; available treatments offer relatively small symptomatic benefit but remain palliative in nature. Current treatments can be divided into pharmaceutical, psychosocial and caregiving.

Molecular structure of
memantine, a medication approved for advanced AD symptoms
Five medications are currently approved by regulatory agencies such as the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) to treat the cognitive manifestations of AD: four are acetylcholinesterase inhibitors (Tacrine, Rivastigmine, Galantamine and Donepezil) and the other (memantine) is an NMDA receptor antagonist. No drug has an indication for delaying or halting the progression of the disease.
Reduction in the activity of the cholinergic neurons is a well-known feature of Alzheimer's disease.[154] Acetylcholinesterase inhibitors are employed to reduce the rate at which acetylcholine (ACh) is broken down, thereby increasing the concentration of ACh in the brain and combating the loss of ACh caused by the death of cholinergic neurons.[155] Cholinesterase inhibitors approved for the management of AD symptoms are donepezil (brand name Aricept),[156] galantamine (Razadyne),[157] and rivastigmine (branded as Exelon[158] and Exelon Patch[159]). There is evidence for the efficacy of these medications in mild to moderate Alzheimer's disease,[160][161] and some evidence for their use in the advanced stage. Only donepezil is approved for treatment of advanced AD dementia.[162] The use of these drugs in mild cognitive impairment has not shown any effect in a delay of the onset of AD.[163] The most common side effects are nausea and vomiting, both of which are linked to cholinergic excess. These side effects arise in approximately 10–20% of users and are mild to moderate in severity. Less common secondary effects include muscle cramps, decreased heart rate (bradycardia), decreased appetite and weight, and increased gastric acid production.[164]
Glutamate is a useful excitatory neurotransmitter of the nervous system, although excessive amounts in the brain can lead to cell death through a process called excitotoxicity which consists of the overstimulation of glutamate receptors. Excitotoxicity occurs not only in Alzheimer's disease, but also in other neurological diseases such as Parkinson's disease and multiple sclerosis.[165] Memantine (brand names Akatinol, Axura, Ebixa/Abixa, Memox and Namenda),[166] is a noncompetitive NMDA receptor antagonist first used as an anti-influenza agent. It acts on the glutamatergic system by blocking NMDA receptors and inhibiting their overstimulation by glutamate.[165] Memantine has been shown to be moderately efficacious in the treatment of moderate to severe Alzheimer's disease. Its effects in the initial stages of AD are unknown.[167] Reported adverse events with memantine are infrequent and mild, including hallucinations, confusion, dizziness, headache and fatigue.[168] The combination of memantine and donepezil has been shown to be "of statistically significant but clinically marginal effectiveness".[169]
Antipsychotic drugs are modestly useful in reducing aggression and psychosis in Alzheimer's disease with behavioural problems, but are associated with serious adverse effects, such as cerebrovascular events, movement difficulties or cognitive decline, that do not permit their routine use.[170][171] When used in the long-term, they have been shown to associate with increased mortality.[171]
People with Alzheimer’s disease who have taken Huperzine A may have improved general cognitive function, global clinical status, functional performance and reduced behavioural disturbance compared to people taking placebos, according to a Cochrane Review, however, the poor methodological quality of the small trials, including problems with blinding and randomisation, led reviewers to conclude "There is currently insufficient evidence of the effects of Huperzine A for Alzheimer's disease (AD)."[172]

A specifically designed room for sensory integration therapy, also called
snoezelen; an emotion-oriented psychosocial intervention for people with dementia
Psychosocial interventions are used as an adjunct to pharmaceutical treatment and can be classified within behaviour-, emotion-, cognition- or stimulation-oriented approaches. Research on efficacy is unavailable and rarely specific to AD, focusing instead on dementia in general.[173]
Behavioural interventions attempt to identify and reduce the antecedents and consequences of problem behaviours. This approach has not shown success in improving overall functioning,[174] but can help to reduce some specific problem behaviours, such as incontinence.[175] There is a lack of high quality data on the effectiveness of these techniques in other behaviour problems such as wandering.[176][177]
Emotion-oriented interventions include reminiscence therapy, validation therapy, supportive psychotherapy, sensory integration, also called snoezelen, and simulated presence therapy. Supportive psychotherapy has received little or no formal scientific study, but some clinicians find it useful in helping mildly impaired people adjust to their illness.[173] Reminiscence therapy (RT) involves the discussion of past experiences individually or in group, many times with the aid of photographs, household items, music and sound recordings, or other familiar items from the past. Although there are few quality studies on the effectiveness of RT, it may be beneficial for cognition and mood.[178] Simulated presence therapy (SPT) is based on attachment theories and involves playing a recording with voices of the closest relatives of the person with Alzheimer's disease. There is partial evidence indicating that SPT may reduce challenging behaviours.[179] Finally, validation therapy is based on acceptance of the reality and personal truth of another's experience, while sensory integration is based on exercises aimed to stimulate senses. There is little evidence to support the usefulness of these therapies.[180][181]
The aim of cognition-oriented treatments, which include reality orientation and cognitive retraining, is the reduction of cognitive deficits. Reality orientation consists in the presentation of information about time, place or person in order to ease the understanding of the person about its surroundings and his or her place in them. On the other hand cognitive retraining tries to improve impaired capacities by exercitation of mental abilities. Both have shown some efficacy improving cognitive capacities,[182][183] although in some studies these effects were transient and negative effects, such as frustration, have also been reported.[173]
Stimulation-oriented treatments include art, music and pet therapies, exercise, and any other kind of recreational activities. Stimulation has modest support for improving behaviour, mood, and, to a lesser extent, function. Nevertheless, as important as these effects are, the main support for the use of stimulation therapies is the change in the person's routine.[173]
Since Alzheimer's has no cure and it gradually renders people incapable of tending for their own needs, caregiving essentially is the treatment and must be carefully managed over the course of the disease.
During the early and moderate stages, modifications to the living environment and lifestyle can increase patient safety and reduce caretaker burden.[184][185] Examples of such modifications are the adherence to simplified routines, the placing of safety locks, the labelling of household items to cue the person with the disease or the use of modified daily life objects.[173][186][187] The patient may also become incapable of feeding themselves, so they require food in smaller pieces or pureed.[188] When swallowing difficulties arise, the use of feeding tubes may be required. In such cases, the medical efficacy and ethics of continuing feeding is an important consideration of the caregivers and family members.[189][190] The use of physical restraints is rarely indicated in any stage of the disease, although there are situations when they are necessary to prevent harm to the person with AD or their caregivers.[173]
As the disease progresses, different medical issues can appear, such as oral and dental disease, pressure ulcers, malnutrition, hygiene problems, or respiratory, skin, or eye infections. Careful management can prevent them, while professional treatment is needed when they do arise.[191][192] During the final stages of the disease, treatment is centred on relieving discomfort until death.[193]
A small recent study in the US concluded that people whose caregivers had a realistic understanding of the prognosis and clinical complications of late dementia were less likely to receive aggressive treatment near the end of life. [194]
There is strong evidence that feeding tubes do not help people with advanced Alzheimer's dementia gain weight, regain strength or function, prevent aspiration pneumonias, or improve quality of life.[195][196][197][198]

Disability-adjusted life year for Alzheimer and other dementias per 100,000 inhabitants in 2004.
no data
≤ 50
50–70
70–90
90–110
110–130
130–150
|
150–170
170–190
190–210
210–230
230–250
≥ 250
|
The early stages of Alzheimer's disease are difficult to diagnose. A definitive diagnosis is usually made once cognitive impairment compromises daily living activities, although the person may still be living independently. The symptoms will progress from mild cognitive problems, such as memory loss through increasing stages of cognitive and non-cognitive disturbances, eliminating any possibility of independent living, especially in the late stages of the disease.[25]
Life expectancy of the population with the disease is reduced.[9][199][200] The mean life expectancy following diagnosis is approximately seven years.[9] Fewer than 3% of people live more than fourteen years.[10] Disease features significantly associated with reduced survival are an increased severity of cognitive impairment, decreased functional level, history of falls, and disturbances in the neurological examination. Other coincident diseases such as heart problems, diabetes or history of alcohol abuse are also related with shortened survival.[199][201][202] While the earlier the age at onset the higher the total survival years, life expectancy is particularly reduced when compared to the healthy population among those who are younger.[200] Men have a less favourable survival prognosis than women.[10][203]
The disease is the underlying cause of death in 70% of all cases.[9] Pneumonia and dehydration are the most frequent immediate causes of death, while cancer is a less frequent cause of death than in the general population.[9][203]
Incidence rates
after age 65[204]
| Age |
New affected
per thousand
person–years |
| 65–69 |
3 |
| 70–74 |
6 |
| 75–79 |
9 |
| 80–84 |
23 |
| 85–89 |
40 |
| 90– |
69 |
Two main measures are used in epidemiological studies: incidence and prevalence. Incidence is the number of new cases per unit of person–time at risk (usually number of new cases per thousand person–years); while prevalence is the total number of cases of the disease in the population at any given time.
Regarding incidence, cohort longitudinal studies (studies where a disease-free population is followed over the years) provide rates between 10 and 15 per thousand person–years for all dementias and 5–8 for AD,[204][205] which means that half of new dementia cases each year are AD. Advancing age is a primary risk factor for the disease and incidence rates are not equal for all ages: every five years after the age of 65, the risk of acquiring the disease approximately doubles, increasing from 3 to as much as 69 per thousand person years.[204][205] There are also sex differences in the incidence rates, women having a higher risk of developing AD particularly in the population older than 85.[205][206]
Prevalence of AD in populations is dependent upon different factors including incidence and survival. Since the incidence of AD increases with age, it is particularly important to include the mean age of the population of interest. In the United States, Alzheimer prevalence was estimated to be 1.6% in 2000 both overall and in the 65–74 age group, with the rate increasing to 19% in the 75–84 group and to 42% in the greater than 84 group.[207] Prevalence rates in less developed regions are lower.[208] The World Health Organization estimated that in 2005, 0.379% of people worldwide had dementia, and that the prevalence would increase to 0.441% in 2015 and to 0.556% in 2030.[209] Other studies have reached similar conclusions.[208] Another study estimated that in 2006, 0.40% of the world population (range 0.17–0.89%; absolute number 26.6 million, range 11.4–59.4 million) were afflicted by AD, and that the prevalence rate would triple and the absolute number would quadruple by 2050.[3]

Alois Alzheimer's patient
Auguste Deter in 1902. Hers was the first described case of what became known as Alzheimer's disease.
The ancient Greek and Roman philosophers and physicians associated old age with increasing dementia.[1] It was not until 1901 that German psychiatrist Alois Alzheimer identified the first case of what became known as Alzheimer's disease in a fifty-year-old woman he called Auguste D. He followed her case until she died in 1906, when he first reported publicly on it.[210] During the next five years, eleven similar cases were reported in the medical literature, some of them already using the term Alzheimer's disease.[1] The disease was first described as a distinctive disease by Emil Kraepelin after suppressing some of the clinical (delusions and hallucinations) and pathological features (arteriosclerotic changes) contained in the original report of Auguste D.[211] He included Alzheimer's disease, also named presenile dementia by Kraepelin, as a subtype of senile dementia in the eighth edition of his Textbook of Psychiatry, published on July 15, 1910.[212]
For most of the 20th century, the diagnosis of Alzheimer's disease was reserved for individuals between the ages of 45 and 65 who developed symptoms of dementia. The terminology changed after 1977 when a conference on AD concluded that the clinical and pathological manifestations of presenile and senile dementia were almost identical, although the authors also added that this did not rule out the possibility that they had different causes.[213] This eventually led to the diagnosis of Alzheimer's disease independently of age.[214] The term senile dementia of the Alzheimer type (SDAT) was used for a time to describe the condition in those over 65, with classical Alzheimer's disease being used for those younger. Eventually, the term Alzheimer's disease was formally adopted in medical nomenclature to describe individuals of all ages with a characteristic common symptom pattern, disease course, and neuropathology.[215]
Dementia, and specifically Alzheimer's disease, may be among the most costly diseases for society in Europe and the United States,[18][19] while their cost in other countries such as Argentina,[216] or South Korea,[217] is also high and rising. These costs will probably increase with the ageing of society, becoming an important social problem. AD-associated costs include direct medical costs such as nursing home care, direct nonmedical costs such as in-home day care, and indirect costs such as lost productivity of both patient and caregiver.[19] Numbers vary between studies but dementia costs worldwide have been calculated around $160 billion,[218] while costs of Alzheimer in the United States may be $100 billion each year.[19]
The greatest origin of costs for society is the long-term care by health care professionals and particularly institutionalisation, which corresponds to 2/3 of the total costs for society.[18] The cost of living at home is also very high,[18] especially when informal costs for the family, such as caregiving time and caregiver's lost earnings, are taken into account.[219]
Costs increase with dementia severity and the presence of behavioural disturbances,[220] and are related to the increased caregiving time required for the provision of physical care.[219] Therefore any treatment that slows cognitive decline, delays institutionalisation or reduces caregivers' hours will have economic benefits. Economic evaluations of current treatments have shown positive results.[19]
The role of the main caregiver is often taken by the spouse or a close relative.[14] Alzheimer's disease is known for placing a great burden on caregivers which includes social, psychological, physical or economic aspects.[15][16][17] Home care is usually preferred by people with AD and their families.[221] This option also delays or eliminates the need for more professional and costly levels of care.[221][222] Nevertheless two-thirds of nursing home residents have dementias.[173]
Dementia caregivers are subject to high rates of physical and mental disorders.[223] Factors associated with greater psychosocial problems of the primary caregivers include having an affected person at home, the carer being a spouse, demanding behaviours of the cared person such as depression, behavioural disturbances, hallucinations, sleep problems or walking disruptions and social isolation.[224][225] Regarding economic problems, family caregivers often give up time from work to spend 47 hours per week on average with the person with AD, while the costs of caring for them are high. Direct and indirect costs of caring for an Alzheimer's patient average between $18,000 and $77,500 per year in the United States, depending on the study.[14][219]
Cognitive behavioural therapy and the teaching of coping strategies either individually or in group have demonstrated their efficacy in improving caregivers' psychological health.[15][226]
As Alzheimer's disease is highly prevalent, many notable people have developed it. Well-known examples are former United States President Ronald Reagan and Irish writer Iris Murdoch, both of whom were the subjects of scientific articles examining how their cognitive capacities deteriorated with the disease.[227][228][229] Other cases include the retired footballer Ferenc Puskas,[230] the former Prime Ministers Harold Wilson (United Kingdom) and Adolfo Suárez (Spain),[231][232] the actress Rita Hayworth,[233] the actor Charlton Heston,[234] the novelist Terry Pratchett,[235] Indian politician George Fernandes,[236] and the 2009 Nobel Prize in Physics recipient Charles K. Kao.[237]
AD has also been portrayed in films such as: Iris (2001), based on John Bayley's memoir of his wife Iris Murdoch;[238] The Notebook (2004), based on Nicholas Sparks' 1996 novel of the same name;[239] A Moment to Remember (2004);Thanmathra (2005);[240] Memories of Tomorrow (Ashita no Kioku) (2006), based on Hiroshi Ogiwara's novel of the same name;[241] Away from Her (2006), based on Alice Munro's short story "The Bear Came over the Mountain".[242] Documentaries on Alzheimer's disease include Malcolm and Barbara: A Love Story (1999) and Malcolm and Barbara: Love's Farewell (2007), both featuring Malcolm Pointon.[243]
As of 2012[update], the safety and efficacy of more than 400 pharmaceutical treatments had been or were being investigated in 1012 clinical trials worldwide, and approximately a quarter of these compounds are in Phase III trials; the last step prior to review by regulatory agencies.[12]
One area of clinical research is focused on treating the underlying disease pathology. Reduction of amyloid beta levels is a common target of compounds[244] (such as apomorphine) under investigation. Immunotherapy or vaccination for the amyloid protein is one treatment modality under study.[245] Unlike preventative vaccination, the putative therapy would be used to treat people already diagnosed. It is based upon the concept of training the immune system to recognise, attack, and reverse deposition of amyloid, thereby altering the course of the disease.[246] An example of such a vaccine under investigation was ACC-001,[247][248] although the trials were suspended in 2008.[249] Another similar agent is bapineuzumab, an antibody designed as identical to the naturally induced anti-amyloid antibody.[250] Other approaches are neuroprotective agents, such as AL-108,[251] and metal-protein interaction attenuation agents, such as PBT2.[252] A TNFα receptor fusion protein, etanercept has showed encouraging results.[253]
In 2008, two separate clinical trials showed positive results in modifying the course of disease in mild to moderate AD with methylthioninium chloride (trade name rember), a drug that inhibits tau aggregation,[254][255] and dimebon, an antihistamine.[256] The consecutive Phase-III trial of Dimebon failed to show positive effects in the primary and secondary endpoints.[257]
The possibility that AD could be treated with antiviral medication is suggested by a study showing colocation of herpes simplex virus with amyloid plaques.[258]
Preliminary research on the effects of meditation on retrieving memory and cognitive functions have been encouraging. Limitations of this research can be addressed in future studies with more detailed analyses.[259]
An FDA panel voted unanimously to recommend approval of florbetapir (tradename: Amyvid), which is currently used in an investigational study. The agent can detect Alzheimer's brain plaques, but will require additional clinical research before it can be made available commercially.[260]
- ↑ 1.0 1.1 1.2 Berchtold NC, Cotman CW. Evolution in the conceptualization of dementia and Alzheimer's disease: Greco-Roman period to the 1960s. Neurobiol. Aging. 1998;19(3):173–89. doi:10.1016/S0197-4580(98)00052-9. PMID 9661992.
- ↑ Brookmeyer R., Gray S., Kawas C.. Projections of Alzheimer's disease in the United States and the public health impact of delaying disease onset. American Journal of Public Health. 1998;88(9):1337–42. doi:10.2105/AJPH.88.9.1337. PMID 9736873.
- ↑ 3.0 3.1 2006 prevalence estimate:
- ↑ "What is Alzheimer's disease?". Alzheimers.org.uk. August 2007. http://www.alzheimers.org.uk/site/scripts/documents_info.php?documentID=100. Retrieved 2008-02-21.
- ↑ 5.0 5.1 5.2 5.3 5.4 5.5 5.6 Waldemar G. Recommendations for the diagnosis and management of Alzheimer's disease and other disorders associated with dementia: EFNS guideline. Eur J Neurol. 2007;14(1):e1–26. doi:10.1111/j.1468-1331.2006.01605.x. PMID 17222085.
- ↑ "Alzheimer's diagnosis of AD". Alzheimer's Research Trust. http://www.alzheimersresearchuk.org/diagnosis/. Retrieved 2008-02-29.
- ↑ Tabert MH, Liu X, Doty RL, Serby M, Zamora D, Pelton GH, Marder K, Albers MW, Stern Y, Devanand DP. A 10-item smell identification scale related to risk for Alzheimer's disease. Ann. Neurol.. 2005;58(1):155–160. doi:10.1002/ana.20533. PMID 15984022.
- ↑ "About Alzheimer's Disease: Symptoms". National Institute on Aging. http://www.nia.nih.gov/alzheimers/topics/symptoms. Retrieved 2011-12-28.
- ↑ 9.0 9.1 9.2 9.3 9.4 Mölsä PK, Marttila RJ, Rinne UK. Survival and cause of death in Alzheimer's disease and multi-infarct dementia. Acta Neurol Scand. 1986;74(2):103–7. doi:10.1111/j.1600-0404.1986.tb04634.x. PMID 3776457.
- ↑ 10.0 10.1 10.2 Mölsä PK, Marttila RJ, Rinne UK. Long-term survival and predictors of mortality in Alzheimer's disease and multi-infarct dementia. ActaNeurol Scand. 1995;91(3):159–64. PMID 7793228.
- ↑ 11.0 11.1 11.2 Tiraboschi P, Hansen LA, Thal LJ, Corey-Bloom J. The importance of neuritic plaques and tangles to the development and evolution of AD. Neurology. 2004;62(11):1984–9. PMID 15184601.
- ↑ 12.0 12.1 "Clinical Trials. Found 1012 studies with search of: alzheimer". US National Institutes of Health. http://www.clinicaltrials.gov/ct2/results?term=alzheimer. Retrieved 2011-01-10.
- ↑ "More research needed on ways to prevent Alzheimer's, panel finds" (PDF). National Institute on Aging. 2006-08-29. http://www.nia.nih.gov/alzheimers/announcements/2010/06/more-research-needed-ways-prevent-alzheimers-panel-finds. Retrieved 2008-02-29.
- ↑ 14.0 14.1 14.2 "The MetLife study of Alzheimer's disease: The caregiving experience" (PDF). MetLife Mature Market Institute. August 2006. http://www.metlife.com/assets/cao/mmi/publications/studies/mmi-alzheimers-disease-caregiving-experience-study.pdf. Retrieved 2011-02-05.
- ↑ 15.0 15.1 15.2 Thompson CA, Spilsbury K, Hall J, Birks Y, Barnes C, Adamson J. Systematic review of information and support interventions for caregivers of people with dementia. BMC Geriatr. 2007;7:18. doi:10.1186/1471-2318-7-18. PMID 17662119.
- ↑ 16.0 16.1 Schneider J, Murray J, Banerjee S, Mann A. EUROCARE: a cross-national study of co-resident spouse carers for people with Alzheimer's disease: I—Factors associated with carer burden. International Journal of Geriatric Psychiatry. 1999;14(8):651–661. doi:10.1002/(SICI)1099-1166(199908)14:8<651::AID-GPS992>3.0.CO;2-B. PMID 10489656.
- ↑ 17.0 17.1 Murray J, Schneider J, Banerjee S, Mann A. EUROCARE: a cross-national study of co-resident spouse carers for people with Alzheimer's disease: II—A qualitative analysis of the experience of caregiving. International Journal of Geriatric Psychiatry. 1999;14(8):662–667. doi:10.1002/(SICI)1099-1166(199908)14:8<662::AID-GPS993>3.0.CO;2-4. PMID 10489657.
- ↑ 18.0 18.1 18.2 18.3 Bonin-Guillaume S, Zekry D, Giacobini E, Gold G, Michel JP. Impact économique de la démence (English: The economical impact of dementia). Presse Med. 2005;34(1):35–41. French. PMID 15685097.
- ↑ 19.0 19.1 19.2 19.3 19.4 Meek PD, McKeithan K, Schumock GT. Economic considerations in Alzheimer's disease. Pharmacotherapy. 1998;18(2 Pt 2):68–73; discussion 79–82. PMID 9543467.
- ↑ 20.0 20.1 20.2 Bäckman L, Jones S, Berger AK, Laukka EJ, Small BJ. Multiple cognitive deficits during the transition to Alzheimer's disease. J Intern Med. 2004;256(3):195–204. doi:10.1111/j.1365-2796.2004.01386.x. PMID 15324363.
- ↑ Nygård L. Instrumental activities of daily living: a stepping-stone towards Alzheimer's disease diagnosis in subjects with mild cognitive impairment?. Acta Neurol Scand. 2003;Suppl(179):42–6. doi:10.1034/j.1600-0404.107.s179.8.x. PMID 12603250.
- ↑ 22.0 22.1 Arnáiz E, Almkvist O. Neuropsychological features of mild cognitive impairment and preclinical Alzheimer's disease. Acta Neurol. Scand., Suppl.. 2003;179:34–41. doi:10.1034/j.1600-0404.107.s179.7.x. PMID 12603249.
- ↑ Landes AM, Sperry SD, Strauss ME, Geldmacher DS. Apathy in Alzheimer's disease. J Am Geriatr Soc. 2001;49(12):1700–7. doi:10.1046/j.1532-5415.2001.49282.x. PMID 11844006.
- ↑ Petersen RC. The current status of mild cognitive impairment—what do we tell our patients?. Nat Clin Pract Neurol. 2007;3(2):60–1. doi:10.1038/ncpneuro0402. PMID 17279076.
- ↑ 25.00 25.01 25.02 25.03 25.04 25.05 25.06 25.07 25.08 25.09 25.10 25.11 25.12 25.13 25.14 25.15 25.16 25.17 25.18 25.19 25.20 25.21 25.22 Förstl H, Kurz A. Clinical features of Alzheimer's disease. European Archives of Psychiatry and Clinical Neuroscience. 1999;249(6):288–290. doi:10.1007/s004060050101. PMID 10653284.
- ↑ Carlesimo GA, Oscar-Berman M. Memory deficits in Alzheimer's patients: a comprehensive review. Neuropsychol Rev. 1992;3(2):119–69. doi:10.1007/BF01108841. PMID 1300219.
- ↑ Jelicic M, Bonebakker AE, Bonke B. Implicit memory performance of patients with Alzheimer's disease: a brief review. International Psychogeriatrics. 1995;7(3):385–392. doi:10.1017/S1041610295002134. PMID 8821346.
- ↑ 28.0 28.1 Taler V, Phillips NA (July 2008). "Language performance in Alzheimer's disease and mild cognitive impairment: a comparative review". J Clin Exp Neuropsychol 30 (5): 501–56. DOI:10.1080/13803390701550128. PMID 18569251.
- ↑ 29.0 29.1 29.2 Frank EM. Effect of Alzheimer's disease on communication function. J S C Med Assoc. 1994;90(9):417–23. PMID 7967534.
- ↑ Volicer L, Harper DG, Manning BC, Goldstein R, Satlin A. Sundowning and circadian rhythms in Alzheimer's disease. Am J Psychiatry. 2001 [cited 2008-08-27];158(5):704–11. doi:10.1176/appi.ajp.158.5.704. PMID 11329390.
- ↑ Gold DP, Reis MF, Markiewicz D, Andres D. When home caregiving ends: a longitudinal study of outcomes for caregivers of relatives with dementia. J Am Geriatr Soc. 1995;43(1):10–6. PMID 7806732.
- ↑ "What We Know Today About Alzheimer's Disease". Alzheimer's Association. http://www.alz.org/research/science/alzheimers_disease_causes.asp. Retrieved 1 October 2011. "While scientists know Alzheimer's disease involves progressive brain cell failure, the reason cells fail isn't clear."
- ↑ "Alzheimer's Disease: Causes". NYU Medical Center/NYU School of Medicine. http://www.med.nyu.edu/adc/forpatients/ad.html#causes. Retrieved 30 September 2011. "The cause of Alzheimer's disease is not yet known, but scientists are hoping to find the answers by studying the characteristic brain changes that occur in a patient with Alzheimer's disease. In rare cases when the disease emerges before the age of sixty-five, these brain changes are caused by a genetic abnormality. Scientists are also looking to genetics as well as environmental factors for possible clues to the cause and cure of Alzheimer's disease."
- ↑ Francis PT, Palmer AM, Snape M, Wilcock GK. The cholinergic hypothesis of Alzheimer's disease: a review of progress. J. Neurol. Neurosurg. Psychiatr.. 1999;66(2):137–47. doi:10.1136/jnnp.66.2.137. PMID 10071091.
- ↑ Shen ZX. Brain cholinesterases: II. The molecular and cellular basis of Alzheimer's disease. Med Hypotheses. 2004;63(2):308–21. doi:10.1016/j.mehy.2004.02.031. PMID 15236795.
- ↑ 36.0 36.1 Wenk GL. Neuropathologic changes in Alzheimer's disease. J Clin Psychiatry. 2003;64 Suppl 9:7–10. PMID 12934968.
- ↑ Hardy J, Allsop D. Amyloid deposition as the central event in the aetiology of Alzheimer's disease. Trends Pharmacol. Sci.. 1991;12(10):383–88. doi:10.1016/0165-6147(91)90609-V. PMID 1763432.
- ↑ 38.0 38.1 Mudher A, Lovestone S. Alzheimer's disease-do tauists and baptists finally shake hands?. Trends Neurosci.. 2002;25(1):22–26. doi:10.1016/S0166-2236(00)02031-2. PMID 11801334.
- ↑ Nistor M. Alpha- and beta-secretase activity as a function of age and beta-amyloid in Down syndrome and normal brain. Neurobiol Aging. 2007;28(10):1493–1506. doi:10.1016/j.neurobiolaging.2006.06.023. PMID 16904243.
- ↑ Lott IT, Head E. Alzheimer disease and Down syndrome: factors in pathogenesis. Neurobiol Aging. 2005;26(3):383–89. doi:10.1016/j.neurobiolaging.2004.08.005. PMID 15639317.
- ↑ Polvikoski T. Apolipoprotein E, dementia, and cortical deposition of beta-amyloid protein. N Engl J Med. 1995;333(19):1242–47. doi:10.1056/NEJM199511093331902. PMID 7566000.
- ↑ Transgenic mice:
- Games D. Alzheimer-type neuropathology in transgenic mice overexpressing V717F beta-amyloid precursor protein. Nature. 1995;373(6514):523–27. doi:10.1038/373523a0. PMID 7845465.
- Masliah E, Sisk A, Mallory M, Mucke L, Schenk D, Games D. Comparison of neurodegenerative pathology in transgenic mice overexpressing V717F beta-amyloid precursor protein and Alzheimer's disease. J Neurosci. 1996;16(18):5795–811. PMID 8795633.
- Hsiao K. Correlative memory deficits, Abeta elevation, and amyloid plaques in transgenic mice. Science. 1996;274(5284):99–102. doi:10.1126/science.274.5284.99. PMID 8810256.
- Lalonde R, Dumont M, Staufenbiel M, Sturchler-Pierrat C, Strazielle C.. Spatial learning, exploration, anxiety, and motor coordination in female APP23 transgenic mice with the Swedish mutation. Brain Research (journal). 2002;956(1):36–44. doi:10.1016/S0006-8993(02)03476-5. PMID 12426044.
- ↑ Holmes C. Long-term effects of Abeta42 immunisation in Alzheimer's disease: follow-up of a randomised, placebo-controlled phase I trial. Lancet. 2008;372(9634):216–23. doi:10.1016/S0140-6736(08)61075-2. PMID 18640458.
- ↑ Lacor PN. Aß Oligomer-Induced Aberrations in Synapse Composition, Shape, and Density Provide a Molecular Basis for Loss of Connectivity in Alzheimer's Disease. Journal of Neuroscience. 2007;27(4):796–807. doi:10.1523/JNEUROSCI.3501-06.2007. PMID 17251419.
- ↑ Lauren J. Cellular Prion Protein Mediates Impairment of Synaptic Plasticity by Amyloid-β Oligomers. Nature. 2009;457(7233):1128–32. doi:10.1038/nature07761. PMID 19242475.
- ↑ 46.0 46.1 Nikolaev A, McLaughlin T, O'Leary D, Tessier-Lavigne M. APP binds DR6 to cause axon pruning and neuron death via distinct caspases. Nature. 19 February 2009;457(7232):981–989. doi:10.1038/nature07767. PMID 19225519.
- ↑ Schmitz C. Hippocampal Neuron Loss Exceeds Amyloid Plaque Load in a Transgenic Mouse Model of Alzheimer's Disease. Am J Pathol. 2004;164(4):1495–1502. doi:10.1016/S0002-9440(10)63235-X. PMID 15039236.
- ↑ Goedert M, Spillantini MG, Crowther RA. Tau proteins and neurofibrillary degeneration. Brain Pathol. 1991;1(4):279–86. doi:10.1111/j.1750-3639.1991.tb00671.x. PMID 1669718.
- ↑ Iqbal K. Tau pathology in Alzheimer disease and other tauopathies. Biochim Biophys Acta. 2005;1739(2–3):198–210. doi:10.1016/j.bbadis.2004.09.008. PMID 15615638.
- ↑ Chun W, Johnson GV. The role of tau phosphorylation and cleavage in neuronal cell death. Front Biosci. 2007;12:733–56. doi:10.2741/2097. PMID 17127334.
- ↑ Itzhaki RF, Wozniak MA. Herpes simplex virus type 1 in Alzheimer's disease: the enemy within. J Alzheimers Dis. 2008 [cited 2011-02-05];13(4):393–405. PMID 18487848.
- ↑ Bartzokis G (August 2011). "Alzheimer's disease as homeostatic responses to age-related myelin breakdown". Neurobiol. Aging 32 (8): 1341–71. DOI:10.1016/j.neurobiolaging.2009.08.007. PMC 3128664. PMID 19775776. //www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=3128664.
- ↑ Bartzokis G, Lu PH, Mintz J (December 2004). "Quantifying age-related myelin breakdown with MRI: novel therapeutic targets for preventing cognitive decline and Alzheimer's disease". J. Alzheimers Dis. 6 (6 Suppl): S53–9. PMID 15665415.
- ↑ Bartzokis G, Lu PH, Mintz J (April 2007). "Human brain myelination and amyloid beta deposition in Alzheimer's disease". Alzheimers Dement 3 (2): 122–5. DOI:10.1016/j.jalz.2007.01.019. PMC 2442864. PMID 18596894. //www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2442864.
- ↑ Su B, Wang X, Nunomura A, et al. (December 2008). "Oxidative stress signaling in Alzheimer's disease". Curr Alzheimer Res 5 (6): 525–32. DOI:10.2174/156720508786898451. PMC 2780015. PMID 19075578. //www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2780015.
- ↑ Kastenholz B, Garfin DE, Horst J, Nagel KA (2009). "Plant metal chaperones: a novel perspective in dementia therapy". Amyloid 16 (2): 81–3. DOI:10.1080/13506120902879392. PMID 20536399.
- ↑ 57.0 57.1 57.2 Heneka MT, Nadrigny F, Regen T, Martinez-Hernandez A, Dumitrescu-Ozimek L, Terwel D, Jardanhazi-Kurutz D, Walter J, Kirchhoff F, Hanisch UK, Kummer MP. (2010). Locus ceruleus controls Alzheimer's disease pathology by modulating microglial functions through norepinephrine. Proc Natl Acad Sci U S A. 107:6058–6063 doi:10.1073/pnas.0909586107 PMID 20231476
- ↑ Desikan RS, Cabral HJ, Hess CP, et al. (August 2009). "Automated MRI measures identify individuals with mild cognitive impairment and Alzheimer's disease". Brain 132 (Pt 8): 2048–57. DOI:10.1093/brain/awp123. PMC 2714061. PMID 19460794. //www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2714061.
- ↑ Moan R. MRI software accurately IDs preclinical Alzheimer's disease. Diagnostic Imaging. July 20, 2009.
- ↑ Bouras C, Hof PR, Giannakopoulos P, Michel JP, Morrison JH. Regional distribution of neurofibrillary tangles and senile plaques in the cerebral cortex of elderly patients: a quantitative evaluation of a one-year autopsy population from a geriatric hospital. Cereb. Cortex. 1994;4(2):138–50. doi:10.1093/cercor/4.2.138. PMID 8038565.
- ↑ Kotzbauer PT, Trojanowsk JQ, Lee VM. Lewy body pathology in Alzheimer's disease. J Mol Neurosci. 2001;17(2):225–32. doi:10.1385/JMN:17:2:225. PMID 11816795.
- ↑ Hashimoto M, Rockenstein E, Crews L, Masliah E. Role of protein aggregation in mitochondrial dysfunction and neurodegeneration in Alzheimer's and Parkinson's diseases. Neuromolecular Med.. 2003;4(1–2):21–36. doi:10.1385/NMM:4:1-2:21. PMID 14528050.
- ↑ Priller C, Bauer T, Mitteregger G, Krebs B, Kretzschmar HA, Herms J. Synapse formation and function is modulated by the amyloid precursor protein. J. Neurosci.. 2006;26(27):7212–21. doi:10.1523/JNEUROSCI.1450-06.2006. PMID 16822978.
- ↑ Turner PR, O'Connor K, Tate WP, Abraham WC. Roles of amyloid precursor protein and its fragments in regulating neural activity, plasticity and memory. Prog. Neurobiol.. 2003;70(1):1–32. doi:10.1016/S0301-0082(03)00089-3. PMID 12927332.
- ↑ Hooper NM. Roles of proteolysis and lipid rafts in the processing of the amyloid precursor protein and prion protein. Biochem. Soc. Trans.. 2005;33(Pt 2):335–8. doi:10.1042/BST0330335. PMID 15787600.
- ↑ Ohnishi S, Takano K. Amyloid fibrils from the viewpoint of protein folding. Cell. Mol. Life Sci.. 2004;61(5):511–24. doi:10.1007/s00018-003-3264-8. PMID 15004691.
- ↑ Hernández F, Avila J. Tauopathies. Cell. Mol. Life Sci.. 2007;64(17):2219–33. doi:10.1007/s00018-007-7220-x. PMID 17604998.
- ↑ Van Broeck B, Van Broeckhoven C, Kumar-Singh S. Current insights into molecular mechanisms of Alzheimer disease and their implications for therapeutic approaches. Neurodegener Dis. 2007;4(5):349–65. doi:10.1159/000105156. PMID 17622778.
- ↑ Yankner BA, Duffy LK, Kirschner DA. Neurotrophic and neurotoxic effects of amyloid beta protein: reversal by tachykinin neuropeptides. Science. 1990;250(4978):279–82. doi:10.1126/science.2218531. PMID 2218531.
- ↑ Chen X, Yan SD. Mitochondrial Abeta: a potential cause of metabolic dysfunction in Alzheimer's disease. IUBMB Life. 2006;58(12):686–94. doi:10.1080/15216540601047767. PMID 17424907.
- ↑ Greig NH. New therapeutic strategies and drug candidates for neurodegenerative diseases: p53 and TNF-alpha inhibitors, and GLP-1 receptor agonists. Ann. N. Y. Acad. Sci.. 2004;1035:290–315. doi:10.1196/annals.1332.018. PMID 15681814.
- ↑ Tapia-Arancibia L, Aliaga E, Silhol M, Arancibia S. New insights into brain BDNF function in normal aging and Alzheimer disease. Brain Research Reviews. 2008;59(1):201–20. doi:10.1016/j.brainresrev.2008.07.007. PMID 18708092.
- ↑ Schindowski K, Belarbi K, Buée L. Neurotrophic factors in Alzheimer's disease: role of axonal transport. Genes, Brain and Behavior. 2008;7(Suppl 1):43–56. doi:10.1111/j.1601-183X.2007.00378.x. PMID 18184369.
- ↑ 74.0 74.1 74.2 Blennow K, de Leon MJ, Zetterberg H. Alzheimer's disease. Lancet. 2006;368(9533):387–403. doi:10.1016/S0140-6736(06)69113-7. PMID 16876668.
- ↑ 75.0 75.1 75.2 Waring SC, Rosenberg RN. Genome-wide association studies in Alzheimer disease. Arch Neurol. 2008;65(3):329–34. doi:10.1001/archneur.65.3.329. PMID 18332245.
- ↑ 76.0 76.1 Selkoe DJ. Translating cell biology into therapeutic advances in Alzheimer's disease. Nature. 1999;399(6738 Suppl):A23–31. doi:10.1038/19866. PMID 10392577.
- ↑ Shioi J. FAD mutants unable to increase neurotoxic Aβ 42 suggest that mutation effects on neurodegeneration may be independent of effects on Abeta. J Neurochem.. 2007;101(3):674–81. doi:10.1111/j.1471-4159.2006.04391.x. PMID 17254019.
- ↑ Strittmatter WJ. Apolipoprotein E: high-avidity binding to beta-amyloid and increased frequency of type 4 allele in late-onset familial Alzheimer disease. Proc. Natl. Acad. Sci. USA. 1993;90(5):1977–81. doi:10.1073/pnas.90.5.1977. PMID 8446617.
- ↑ 79.0 79.1 Mahley RW, Weisgraber KH, Huang Y. Apolipoprotein E4: A causative factor and therapeutic target in neuropathology, including Alzheimer's disease. Proc. Natl. Acad. Sci. U.S.A.. 2006;103(15):5644–51. doi:10.1073/pnas.0600549103. PMID 16567625.
- ↑ Hall K, Murrell J, Ogunniyi A, Deeg M, Baiyewu O, Gao S, Gureje O, Dickens J, Evans R, Smith-Gamble V, Unverzagt FW, Shen J, Hendrie H. Cholesterol, APOE genotype, and Alzheimer disease: An epidemiologic study of Nigerian Yoruba. Neurology. 2006;66(2):223–227. doi:10.1212/01.wnl.0000194507.39504.17. PMID 16434658. PMC 2860622.
- ↑ Gureje O, Ogunniyi A, Baiyewu O, Price B, Unverzagt FW, Evans RM, Smith-Gamble V, Lane KA, Gao S, Hall KS, Hendrie HC, Murrell JR. APOE ε4 Is Not Associated with Alzheimer's Disease in Elderly Nigerians. Ann Neurol. 2006;59(1):182–185. doi:10.1002/ana.20694. PMID 16278853. PMC 2855121.
- ↑ Mendez MF. The accurate diagnosis of early-onset dementia. International Journal of Psychiatry Medicine. 2006;36(4):401–412. doi:10.2190/Q6J4-R143-P630-KW41. PMID 17407994.
- ↑ Klafki HW, Staufenbiel M, Kornhuber J, Wiltfang J. Therapeutic approaches to Alzheimer's disease. Brain. 2006;129(Pt 11):2840–55. doi:10.1093/brain/awl280. PMID 17018549.
- ↑ (PDF) Dementia: Quick reference guide. London: (UK) National Institute for Health and Clinical Excellence. November 2006. ISBN 1-84629-312-X. http://www.nice.org.uk/nicemedia/pdf/CG042quickrefguide.pdf. Retrieved 2008-02-22.
- ↑ 85.0 85.1 Schroeter ML, Stein T, Maslowski N, Neumann J. Neural Correlates of Alzheimer's Disease and Mild Cognitive Impairment: A Systematic and Quantitative Meta-Analysis involving 1,351 Patients. NeuroImage. 2009;47(4):1196–1206. doi:10.1016/j.neuroimage.2009.05.037. PMID 19463961.
- ↑ 86.0 86.1 McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer's disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology. 1984;34(7):939–44. PMID 6610841.
- ↑ 87.0 87.1 Dubois B. Research criteria for the diagnosis of Alzheimer's disease: revising the NINCDS-ADRDA criteria. Lancet Neurol. 2007;6(8):734–46. doi:10.1016/S1474-4422(07)70178-3. PMID 17616482.
- ↑ Blacker D, Albert MS, Bassett SS, Go RC, Harrell LE, Folstein MF. Reliability and validity of NINCDS-ADRDA criteria for Alzheimer's disease. The National Institute of Mental Health Genetics Initiative. Arch. Neurol.. 1994;51(12):1198–204. PMID 7986174.
- ↑ American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders: DSM-IV-TR (4th Edition Text Revision ed.). Washington, DC: American Psychiatric Association. ISBN 0-89042-025-4.
- ↑ Ito N. [Clinical aspects of dementia]. Hokkaido Igaku Zasshi. 1996;71(3):315–20. Japanese. PMID 8752526.
- ↑ Tombaugh TN, McIntyre NJ. The mini-mental state examination: a comprehensive review. J Am Geriatr Soc. 1992;40(9):922–35. PMID 1512391.
- ↑ Pasquier F. Early diagnosis of dementia: neuropsychology. J. Neurol.. 1999;246(1):6–15. doi:10.1007/s004150050299. PMID 9987708.
- ↑ Antoine C, Antoine P, Guermonprez P, Frigard B. [Awareness of deficits and anosognosia in Alzheimer's disease.]. Encephale. 2004;30(6):570–7. French. doi:10.1016/S0013-7006(04)95472-3. PMID 15738860.
- ↑ Cruz VT, Pais J, Teixeira A, Nunes B. [The initial symptoms of Alzheimer disease: caregiver perception]. Acta Med Port. 2004;17(6):435–44. Portuguese. PMID 16197855.
- ↑ Marksteiner J, Hinterhuber H, Humpel C. Cerebrospinal fluid biomarkers for diagnosis of Alzheimer's disease: beta-amyloid(1–42), tau, phospho-tau-181 and total protein. Drugs Today. 2007;43(6):423–31. doi:10.1358/dot.2007.43.6.1067341. PMID 17612711.
- ↑ 96.0 96.1 96.2 De Meyer G, Shapiro F, Vanderstichele H, Vanmechelen E, Engelborghs S, De Deyn PP, Coart E, Hansson O, Minthon L, Zetterberg H, Blennow K, Shaw L, Trojanowski JQ. Diagnosis-Independent Alzheimer Disease Biomarker Signature in Cognitively Normal Elderly People. Arch Neurol.. 2010;67(8):949–56. doi:10.1001/archneurol.2010.179. PMID 20697045.
- ↑ Kolata G (August 9, 2010). "Spinal-Fluid Test Is Found to Predict Alzheimer's". The New York Times. http://www.nytimes.com/2010/08/10/health/research/10spinal.html. Retrieved August 10, 2010.
- ↑ Roan S (August 9, 2010). "Tapping into an accurate diagnosis of Alzheimer's disease". Los Angeles Times. http://www.latimes.com/health/boostershots/aging/la-heb-alzheimers-20100809,0,5683387.story. Retrieved August 10, 2010.
- ↑ Clarfield AM. The decreasing prevalence of reversible dementias: an updated meta-analysis. Arch. Intern. Med.. 2003;163(18):2219–29. doi:10.1001/archinte.163.18.2219. PMID 14557220.
- ↑ Sun x. Amyloid-Associated Depression: A Prodromal Depression of Alzheimer Disease?. Arch Gen Psychiatry. 2008;65(5):542–550. doi:10.1001/archpsyc.65.5.542. PMID 18458206. PMC 3042807.
- ↑ Geldmacher DS, Whitehouse PJ. Differential diagnosis of Alzheimer's disease. Neurology. 1997;48(5 Suppl 6):S2–9. PMID 9153154.
- ↑ Potter GG, Steffens DC. Contribution of depression to cognitive impairment and dementia in older adults. Neurologist. 2007;13(3):105–17. doi:10.1097/01.nrl.0000252947.15389.a9. PMID 17495754.
- ↑ Bonte FJ, Harris TS, Hynan LS, Bigio EH, White CL. Tc-99m HMPAO SPECT in the differential diagnosis of the dementias with histopathologic confirmation. Clin Nucl Med. 2006;31(7):376–8. doi:10.1097/01.rlu.0000222736.81365.63. PMID 16785801.
- ↑ Dougall NJ, Bruggink S, Ebmeier KP. Systematic review of the diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia. Am J Geriatr Psychiatry. 2004;12(6):554–70. doi:10.1176/appi.ajgp.12.6.554. PMID 15545324.
- ↑ PiB PET:
- ↑ Abella HA. Report from SNM: PET imaging of brain chemistry bolsters characterization of dementias. Diagnostic Imaging. June 16, 2009.
- ↑ Carpenter AP Jr, Pontecorvo MJ, Hefti FF, Skovronsky DM. The use of the exploratory IND in the evaluation and development of 18F-PET radiopharmaceuticals for amyloid imaging in the brain: a review of one company's experience. Q J Nucl Med Mol Imaging. 2009 Aug;53(4):387–93. PMID 19834448.
- ↑ Leung K (April 8, 2010). "(E)-4-(2-(6-(2-(2-(2-(18F-fluoroethoxy)ethoxy)ethoxy)pyridin-3-yl)vinyl)-N-methyl benzenamine [[18F]AV-45]". Molecular Imaging and Contrast Agent Database. http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=micad&part=AV-45-18F. Retrieved 2010-06-24.
- ↑ Kolata G (June 23, 2010). "Promise Seen for Detection of Alzheimer's". The New York Times. http://www.nytimes.com/2010/06/24/health/research/24scans.html. Retrieved June 23, 2010.
- ↑ 110.0 110.1 Wong DF, Rosenberg PB, Zhou Y, Kumar A, Raymont V, Ravert HT, Dannals RF, Nandi A, Brasić JR, Ye W, Hilton J, Lyketsos C, Kung HF, Joshi AD, Skovronsky DM, Pontecorvo MJ. In Vivo Imaging of Amyloid Deposition in Alzheimer's Disease using the Novel Radioligand 18FAV-45 (Florbetapir F 18). J Nucl Med. 2010 Jun;51(6):913–20. doi:10.2967/jnumed.109.069088. PMID 20501908. Lay summary.
- ↑ Rabinovici GD, Jagust WJ. AMYLOID IMAGING IN AGING AND DEMENTIA: TESTING THE AMYLOID HYPOTHESIS IN VIVO. Behav Neurol. 2009;21(1):117–28. doi:10.3233/BEN-2009-0232. PMID 19847050. PMC 2804478.
- ↑ O'Brien JT. Role of imaging techniques in the diagnosis of dementia. Br J Radiol. 2007 Dec;80(Spec No 2):S71–7. doi:10.1259/bjr/33117326. PMID 18445747.
- ↑ Rupsingh R, Borrie M, Smith M, Wells JL, Bartha R. Reduced hippocampal glutamate in Alzheimer disease. Neurobiol Aging. 2009;32(5):802–810. doi:10.1016/j.neurobiolaging.2009.05.002. PMID 19501936. (primary source)
- ↑ Reddy MM, Wilson R, Wilson J, Connell S, Gocke A, Hynan L, German D, Kodadek T. Identification of Candidate IgG Antibody Biomarkers for Alzheimer's Disease Through Screening of Synthetic Combinatorial Libraries. Cell. 2011;144(1):132–42. doi:10.1016/j.cell.2010.11.054. PMID 21215375. (primary source)
- ↑ Rammouz G, Lecanu L, Aisen P, Papadopoulos V. A lead study on oxidative stress-mediated dehydroepiandrosterone formation in serum: the biochemical basis for a diagnosis of Alzheimer's disease. J Alzheimers Dis. 2011-01-01;24(1):5–16. doi:10.3233/JAD-2011-101941. PMID 21335661. (primary source)
- ↑ Prevention recommendations not supported:
- ↑ Szekely CA, Breitner JC, Zandi PP. Prevention of Alzheimer's disease. Int Rev Psychiatry. 2007;19(6):693–706. doi:10.1080/09540260701797944. PMID 18092245.
- ↑ Patterson C, Feightner JW, Garcia A, Hsiung GY, MacKnight C, Sadovnick AD. Diagnosis and treatment of dementia: 1. Risk assessment and primary prevention of Alzheimer disease. CMAJ. 2008;178(5):548–56. doi:10.1503/cmaj.070796. PMID 18299540.
- ↑ Rosendorff C, Beeri MS, Silverman JM. Cardiovascular risk factors for Alzheimer's disease. Am J Geriatr Cardiol. 2007;16(3):143–9. doi:10.1111/j.1076-7460.2007.06696.x. PMID 17483665.
- ↑ Reiss AB, Wirkowski E. Role of HMG-CoA reductase inhibitors in neurological disorders: progress to date. Drugs. 2007;67(15):2111–20. doi:10.2165/00003495-200767150-00001. PMID 17927279.
- ↑ Kuller LH. Statins and dementia. Curr Atheroscler Rep. 2007;9(2):154–61. doi:10.1007/s11883-007-0012-9. PMID 17877925.
- ↑ 122.0 122.1 Solfrizzi V. Lifestyle-related factors in predementia and dementia syndromes. Expert Rev Neurother. 2008;8(1):133–58. doi:10.1586/14737175.8.1.133. PMID 18088206.
- ↑ Panza F, Capurso C, D'Introno A, Colacicco AM, Frisardi V, Lorusso M, Santamato A, Seripa D, Pilotto A, Scafato E, Vendemiale G, Capurso A, Solfrizzi V.. Alcohol drinking, cognitive functions in older age, predementia, and dementia syndromes. J Alzheimers Dis. May 2009;17(1):7–31. doi:10.3233/JAD-2009-1009. PMID 19494429.
- ↑ 124.0 124.1 124.2 Boothby LA, Doering PL. Vitamin C and vitamin E for Alzheimer's disease. Ann Pharmacother. 2005;39(12):2073–80. doi:10.1345/aph.1E495. PMID 16227450.
- ↑ Isaac MG, Quinn R, Tabet N. Vitamin E for Alzheimer's disease and mild cognitive impairment. Cochrane Database Syst Rev. 2008;(3):CD002854. doi:10.1002/14651858.CD002854.pub2. PMID 18646084.
- ↑ Malouf R, Grimley Evans J. Folic acid with or without vitamin B12 for the prevention and treatment of healthy elderly and demented people. Cochrane Database Syst Rev. 2008;(4):CD004514. doi:10.1002/14651858.CD004514.pub2. PMID 18843658.
- ↑ Wald DS, Kasturiratne A, Simmonds M. Effect of folic acid, with or without other B vitamins, on cognitive decline: meta-analysis of randomized trials. The American Journal of Medicine. June 2010;123(6):522–527.e2. doi:10.1016/j.amjmed.2010.01.017. PMID 20569758.
- ↑ Quinn JF. Docosahexaenoic acid supplementation and cognitive decline in Alzheimer disease: a randomized trial. JAMA. 2010;304(17):1903–11. doi:10.1001/jama.2010.1510. PMID 21045096.
- ↑ 129.0 129.1 129.2 Szekely CA, Town T, Zandi PP. NSAIDs for the chemoprevention of Alzheimer's disease. Subcell Biochem. 2007;42:229–48. doi:10.1007/1-4020-5688-5_11. PMID 17612054.
- ↑ Ringman JM, Frautschy SA, Cole GM, Masterman DL, Cummings JL. A Potential Role of the Curry Spice Curcumin in Alzheimer's Disease. Curr Alzheimer Res. 2005;2(2):131–6. doi:10.2174/1567205053585882. PMID 15974909.
- ↑ Aggarwal BB, Harikumar KB. Potential Therapeutic Effects of Curcumin, the Anti-inflammatory Agent, Against Neurodegenerative, Cardiovascular, Pulmonary, Metabolic, Autoimmune and Neoplastic Diseases. Int J Biochem Cell Biol. 2009;41(1):40–59. doi:10.1016/j.biocel.2008.06.010. PMID 18662800.
- ↑ Farquhar C, Marjoribanks J, Lethaby A, Suckling JA, Lamberts Q. Long term hormone therapy for perimenopausal and postmenopausal women. Cochrane Database Syst Rev. 15 April 2009;(2):CD004143. doi:10.1002/14651858.CD004143.pub3. PMID 19370593.
- ↑ Barrett-Connor E, Laughlin GA. Endogenous and Exogenous Estrogen, Cognitive Function and Dementia in Postmenopausal Women: Evidence from Epidemiologic Studies and Clinical Trials. Semin Reprod Med. May 2009;27(3):275–82. doi:10.1055/s-0029-1216280. PMID 19401958.
- ↑ Birks J, Grimley Evans J. Ginkgo biloba for cognitive impairment and dementia. Cochrane Database Syst Rev. 2009 [cited 2009-08-13];(1):CD003120. doi:10.1002/14651858.CD003120.pub3. PMID 19160216.
- ↑ DeKosky ST. Ginkgo biloba for Prevention of Dementia: A Randomized Controlled Trial. Journal of the American Medical Association. 2008 [cited 2008-11-18];300(19):2253–2262. doi:10.1001/jama.2008.683. PMID 19017911. PMC 2823569.
- ↑ Eskelinen MH, Ngandu T, Tuomilehto J, Soininen H, Kivipelto M. Midlife coffee and tea drinking and the risk of late-life dementia: a population-based CAIDE study. J Alzheimers Dis. 2009;16(1):85–91. doi:10.3233/JAD-2009-0920. PMID 19158424.
- ↑ 137.0 137.1 Stern Y (July 2006). "Cognitive reserve and Alzheimer disease". Alzheimer Disease and Associated Disorders 20 (2): 112–117. DOI:10.1097/01.wad.0000213815.20177.19. ISSN 0893-0341. PMID 16917199. edit
- ↑ 138.0 138.1 Paradise M, Cooper C, Livingston G. Systematic review of the effect of education on survival in Alzheimer's disease. Int Psychogeriatr. 2009;21(1):25–32. doi:10.1017/S1041610208008053. PMID 19026089.
- ↑ "Most Popular E-mail Newsletter". USA Today. http://yourlife.usatoday.com/health/medical/alzheimers/story/2011/02/Speaking-2-languages-may-delay-getting-Alzheimers/43903878/1?csp=34news&utm_source=feedburner&utm_medium=feed&utm_campaign=Feed%3A+usatoday-NewsTopStories+%28News+-+Top+Stories%29.
- ↑ Eubanks LM. A Molecular Link Between the Active Component of Marijuana and Alzheimer's Disease Pathology [Free full text]. Molecular Pharmaceutics. 2006;3(6):773–7. doi:10.1021/mp060066m. PMID 17140265.
- ↑ Campbell VA, Gowran A. Alzheimer's disease; taking the edge off with cannabinoids?. Br J Pharmacol. 2007 November;152(5):655–62. doi:10.1038/sj.bjp.0707446. PMID 17828287.
- ↑ Krishnan, S.; Cairns, R.; Howard, R. (2009). Cannabinoids for the treatment of dementia. In Krishnan, Sarada. "Cochrane Database of Systematic Reviews". Cochrane database of systematic reviews (Online) (2): CD007204. DOI:10.1002/14651858.CD007204.pub2. PMID 19370677. edit
- ↑ Shcherbatykh I, Carpenter DO. The role of metals in the etiology of Alzheimer's disease. J Alzheimers Dis. 2007;11(2):191–205. PMID 17522444.
- ↑ Rondeau V, Commenges D, Jacqmin-Gadda H, Dartigues JF. Relation between aluminum concentrations in drinking water and Alzheimer's disease: an 8-year follow-up study. Am J Epidemiol. 2000;152(1):59–66. doi:10.1093/aje/152.1.59. PMID 10901330.
- ↑ Kukull WA. Solvent exposure as a risk factor for Alzheimer's disease: a case-control study. Am J Epidemiol. 1995;141(11):1059–71; discussion 1072–9. PMID 7771442.
- ↑ Santibáñez M, Bolumar F, García AM. Occupational risk factors in Alzheimer's disease: a review assessing the quality of published epidemiological studies. Occupational and Environmental Medicine. 2007;64(11):723–732. doi:10.1136/oem.2006.028209. PMID 17525096.
- ↑ Seidler A. Occupational exposure to low frequency magnetic fields and dementia: a case–control study. Occup Environ Med. 2007;64(2):108–14. doi:10.1136/oem.2005.024190. PMID 17043077.
- ↑ Rondeau V. A review of epidemiologic studies on aluminum and silica in relation to Alzheimer's disease and associated disorders. Rev Environ Health. 2002;17(2):107–21. doi:10.1515/REVEH.2002.17.2.107. PMID 12222737.
- ↑ Martyn CN, Coggon DN, Inskip H, Lacey RF, Young WF. Aluminum concentrations in drinking water and risk of Alzheimer's disease. Epidemiology. 1997;8(3):281–6. doi:10.1097/00001648-199705000-00009. PMID 9115023.
- ↑ Graves AB, Rosner D, Echeverria D, Mortimer JA, Larson EB. Occupational exposures to solvents and aluminium and estimated risk of Alzheimer's disease. Occup Environ Med. 1998;55(9):627–33. doi:10.1136/oem.55.9.627. PMID 9861186.
- ↑ Scientific Committee on Emerging and Newly Identified Health Risks-SCENIHR. Health Effects of Exposure to EMF. January 2009 [cited 2010-04-27]:4–5.
- ↑ Cataldo JK, Prochaska JJ, Glantz SA. Cigarette smoking is a risk factor for Alzheimer's disease: An analysis controlling for tobacco industry affiliation. J Alzheimers Dis. 2010;19(2):465–80. doi:10.3233/JAD-2010-1240. PMID 20110594.
- ↑ Neuroinflammation – an early event in both the history and pathogenesis of Alzheimer's disease. Neuro-degenerative diseases. 2010;7(1–3):38–41. doi:10.1159/000283480. PMID 20160456.
- ↑ Geula C, Mesulam MM. Cholinesterases and the pathology of Alzheimer disease. Alzheimer Dis Assoc Disord. 1995;9 Suppl 2:23–28. PMID 8534419.
- ↑ Stahl SM. The new cholinesterase inhibitors for Alzheimer's disease, Part 2: illustrating their mechanisms of action. J Clin Psychiatry. 2000;61(11):813–814. doi:10.4088/JCP.v61n1101. PMID 11105732.
- ↑ "Donepezil". Medline Plus. US National Library of Medicine. 2007-01-08. http://www.nlm.nih.gov/medlineplus/druginfo/meds/a697032.html. Retrieved 2010-02-03.
- ↑ "Galantamine". Medline Plus. US National Library of Medicine. 2007-01-08. http://www.nlm.nih.gov/medlineplus/druginfo/meds/a699058.html. Retrieved 2010-02-03.
- ↑ "Rivastigmine". Medline Plus. US National Library of Medicine. 2007-01-08. http://www.nlm.nih.gov/medlineplus/druginfo/meds/a602009.html. Retrieved 2010-02-03.
- ↑ "Rivastigmine Transdermal". Medline Plus. US National Library of Medicine. 2007-01-08. http://www.nlm.nih.gov/medlineplus/druginfo/meds/a607078.html. Retrieved 2010-02-03.
- ↑ Birks J. Cholinesterase inhibitors for Alzheimer's disease. Cochrane Database Syst Rev. 2006;(1):CD005593. doi:10.1002/14651858.CD005593. PMID 16437532.
- ↑ Birks J, Grimley Evans J, Iakovidou V, Tsolaki M, Holt FE. Rivastigmine for Alzheimer's disease. Cochrane Database Syst Rev. 2009-04-15;(2):CD001191. doi:10.1002/14651858.CD001191.pub2. PMID 19370562.
- ↑ Birks J, Harvey RJ. Donepezil for dementia due to Alzheimer's disease. Cochrane Database Syst Rev. 2006-01-25;(1):CD001190. doi:10.1002/14651858.CD001190.pub2. PMID 16437430.
- ↑ Raschetti R, Albanese E, Vanacore N, Maggini M. Cholinesterase Inhibitors in Mild Cognitive Impairment: A Systematic Review of Randomised Trials. PLoS Med. 2007;4(11):e338. doi:10.1371/journal.pmed.0040338. PMID 18044984.
- ↑ Birks J (2006). "Cholinesterase inhibitors for Alzheimer's disease". Cochrane Database Syst Rev (1): CD005593. DOI:10.1002/14651858.CD005593. PMID 16437532.
- ↑ 165.0 165.1 Lipton SA. Paradigm shift in neuroprotection by NMDA receptor blockade: memantine and beyond. Nat Rev Drug Discov. 2006;5(2):160–170. doi:10.1038/nrd1958. PMID 16424917.
- ↑ "Memantine". US National Library of Medicine (Medline). 2004-01-04. http://www.nlm.nih.gov/medlineplus/druginfo/meds/a604006.html. Retrieved 2010-02-03.
- ↑ Areosa Sastre A, McShane R, Sherriff F. Memantine for dementia. Cochrane Database Syst Rev. 2004;(4):CD003154. doi:10.1002/14651858.CD003154.pub2. PMID 15495043.
- ↑ "Namenda Prescribing Information" (PDF). Forest Pharmaceuticals. http://www.frx.com/pi/namenda_pi.pdf. Retrieved 2008-02-19. (primary source)
- ↑ Raina P. Effectiveness of cholinesterase inhibitors and memantine for treating dementia: evidence review for a clinical practice guideline. Annals of Internal Medicine. 2008;148(5):379–397. PMID 18316756.
- ↑ Antipsychotics use:
- ↑ 171.0 171.1 Ballard C, Hanney ML, Theodoulou M, Douglas S, McShane R, Kossakowski K, Gill R, Juszczak E, Yu L-M, Jacoby R. The dementia antipsychotic withdrawal trial (DART-AD): long-term follow-up of a randomised placebo-controlled trial. Lancet Neurology. 9 January 2009;8(2):151–7. doi:10.1016/S1474-4422(08)70295-3. PMID 19138567. Lay summary.
- ↑ Li J, Wu HM, Zhou RL, Liu GJ, Dong BR. Huperzine A for Alzheimer's disease. Cochrane Database Syst Rev. 2008;(2):CD005592. doi:10.1002/14651858.CD005592.pub2. PMID 18425924.
- ↑ 173.0 173.1 173.2 173.3 173.4 173.5 173.6 "Practice Guideline for the Treatment of Patients with Alzheimer's disease and Other Dementias" (PDF). American Psychiatric Association. October 2007. DOI:10.1176/appi.books.9780890423967.152139. http://www.psychiatryonline.com/pracGuide/loadGuidelinePdf.aspx?file=AlzPG101007. Retrieved 2007-12-28.
- ↑ Bottino CM. Cognitive rehabilitation combined with drug treatment in Alzheimer's disease patients: a pilot study. Clin Rehabil. 2005;19(8):861–869. doi:10.1191/0269215505cr911oa. PMID 16323385.
- ↑ Doody RS. Practice parameter: management of dementia (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2001;56(9):1154–1166. PMID 11342679.
- ↑ Hermans DG, Htay UH, McShane R. Non-pharmacological interventions for wandering of people with dementia in the domestic setting. Cochrane Database Syst Rev. 2007;(1):CD005994. doi:10.1002/14651858.CD005994.pub2. PMID 17253573.
- ↑ Robinson L, Hutchings D, Dickinson HO et al.. Effectiveness and acceptability of non-pharmacological interventions to reduce wandering in dementia: a systematic review. Int J Geriatr Psychiatry. 2007;22(1):9–22. doi:10.1002/gps.1643. PMID 17096455.
- ↑ Woods B, Spector A, Jones C, Orrell M, Davies S. Reminiscence therapy for dementia. Cochrane Database Syst Rev. 2005;(2):CD001120. doi:10.1002/14651858.CD001120.pub2. PMID 15846613.
- ↑ Zetteler J. Effectiveness of simulated presence therapy for individuals with dementia: a systematic review and meta-analysis. Aging Ment Health. 2008;12(6):779–85. doi:10.1080/13607860802380631. PMID 19023729.
- ↑ Neal M, Briggs M. Validation therapy for dementia. Cochrane Database Syst Rev. 2003;(3):CD001394. doi:10.1002/14651858.CD001394. PMID 12917907.
- ↑ Chung JC, Lai CK, Chung PM, French HP. Snoezelen for dementia. Cochrane Database Syst Rev. 2002;(4):CD003152. doi:10.1002/14651858.CD003152. PMID 12519587.
- ↑ Spector A, Orrell M, Davies S, Woods B. Withdrawn: Reality orientation for dementia. Cochrane Database Syst Rev. 2000;(3):CD001119. doi:10.1002/14651858.CD001119.pub2. PMID 17636652.
- ↑ Spector A, Thorgrimsen L, Woods B et al.. Efficacy of an evidence-based cognitive stimulation therapy programme for people with dementia: randomised controlled trial. Br J Psychiatry. 2003;183(3):248–254. doi:10.1192/bjp.183.3.248. PMID 12948999.
- ↑ Gitlin LN, Corcoran M, Winter L, Boyce A, Hauck WW. A randomized, controlled trial of a home environmental intervention: effect on efficacy and upset in caregivers and on daily function of persons with dementia. Gerontologist. 1 February 2001 [cited 2008-07-15];41(1):4–14. doi:10.1093/geront/41.1.4. PMID 11220813.
- ↑ Gitlin LN, Hauck WW, Dennis MP, Winter L. Maintenance of effects of the home environmental skill-building program for family caregivers and individuals with Alzheimer's disease and related disorders. J. Gerontol. A Biol. Sci. Med. Sci.. 2005;60(3):368–74. doi:10.1093/gerona/60.3.368. PMID 15860476.
- ↑ "Treating behavioral and psychiatric symptoms". Alzheimer's Association. 2006. Archived from the original on 2006-09-25. http://web.archive.org/web/20060925112503/http://www.alz.org/Health/Treating/agitation.asp. Retrieved 2006-09-25.
- ↑ Dunne TE, Neargarder SA, Cipolloni PB, Cronin-Golomb A. Visual contrast enhances food and liquid intake in advanced Alzheimer's disease. Clinical Nutrition. 2004;23(4):533–538. doi:10.1016/j.clnu.2003.09.015. PMID 15297089.
- ↑ Dudek, Susan G. (2007). Nutrition essentials for nursing practice. Hagerstown, Maryland: Lippincott Williams & Wilkins. p. 360. ISBN 0-7817-6651-6. http://books.google.com/?id=01zo6yf0IUEC&pg=PA360&dq=alzheimer%27s+chew. Retrieved 2008-08-19.
- ↑ Dennehy C. Analysis of patients' rights: dementia and PEG insertion. Br J Nurs. 2006;15(1):18–20. PMID 16415742.
- ↑ Chernoff R. Tube feeding patients with dementia. Nutr Clin Pract. 2006;21(2):142–6. doi:10.1177/0115426506021002142. PMID 16556924.
- ↑ Gambassi G, Landi F, Lapane KL, Sgadari A, Mor V, Bernabei R. Predictors of mortality in patients with Alzheimer's disease living in nursing homes. J. Neurol. Neurosurg. Psychiatr.. 1999;67(1):59–65. doi:10.1136/jnnp.67.1.59. PMID 10369823.
- ↑ Medical issues:
- Head B. Palliative care for persons with dementia. Home Healthc Nurse. 2003;21(1):53–60; quiz 61. doi:10.1097/00004045-200301000-00012. PMID 12544465.
- Friedlander AH, Norman DC, Mahler ME, Norman KM, Yagiela JA. Alzheimer's disease: psychopathology, medical management and dental implications. J Am Dent Assoc. 2006;137(9):1240–51. PMID 16946428.
- Belmin J. Practical guidelines for the diagnosis and management of weight loss in Alzheimer's disease: a consensus from appropriateness ratings of a large expert panel. J Nutr Health Aging. 2007;11(1):33–7. PMID 17315078.
- McCurry SM, Gibbons LE, Logsdon RG, Vitiello M, Teri L. Training caregivers to change the sleep hygiene practices of patients with dementia: the NITE-AD project. J Am Geriatr Soc. 2003;51(10):1455–60. doi:10.1046/j.1532-5415.2003.51466.x. PMID 14511168.
- Perls TT, Herget M. Higher respiratory infection rates on an Alzheimer's special care unit and successful intervention. J Am Geriatr Soc. 1995;43(12):1341–4. PMID 7490383.
- ↑ Shega JW. Palliative Excellence in Alzheimer Care Efforts (PEACE): a program description. J Palliat Med. 2003;6(2):315–20. doi:10.1089/109662103764978641. PMID 12854952.
- ↑ Mitchell SL. The Clinical Course of Advanced Dementia. N Engl J Med. 2009;361(16):1529–38. doi:10.1056/NEJMoa0902234. PMID 19828530.
- ↑ Tube Feeding in Patients With Advanced Dementia, October 13, 1999, Finucane et al. 282 (14): 1365 — JAMA. JAMA : the journal of the American Medical Association. 1999-10-13 [cited 2011-06-16];282(14):1365–70. doi:10.1001/jama.282.14.1365. PMID 10527184.
- ↑ Arch Intern Med – Abstract: The Risk Factors and Impact on Survival of Feeding Tube Placement in Nursing Home Residents With Severe Cognitive Impairment, 10 FEBRUARY 1997, Mitchell et al. 157 (3): 327. 1997-02-10 [cited 2011-06-16]. doi:10.1001/archinte.1997.00440240091014.
- ↑ Arch Intern Med – Abstract: High Short-term Mortality in Hospitalized Patients With Advanced Dementia: Lack of Benefit of Tube Feeding, February 26, 2001, Meier et al. 161 (4): 594. Archives of Internal Medicine. 2001-02-26 [cited 2011-06-16];161(4):594–9. doi:10.1001/archinte.161.4.594. PMID 11252121.
- ↑ "Feeding Tubes in Patients with Severe Dementia". Drplace.com. 2002-04-15. http://www.drplace.com/Feeding_Tubes_in_Patients_with_Severe_Dementia.16.28273.htm. Retrieved 2011-06-16.
- ↑ 199.0 199.1 Bowen JD. Predictors of mortality in patients diagnosed with probable Alzheimer's disease. Neurology. 1996;47(2):433–9. PMID 8757016.
- ↑ 200.0 200.1 Dodge HH, Shen C, Pandav R, DeKosky ST, Ganguli M. Functional transitions and active life expectancy associated with Alzheimer disease. Arch. Neurol.. 2003;60(2):253–9. doi:10.1001/archneur.60.2.253. PMID 12580712.
- ↑ Larson EB. Survival after initial diagnosis of Alzheimer disease. Ann. Intern. Med.. 2004;140(7):501–9. PMID 15068977.
- ↑ Jagger C, Clarke M, Stone A. Predictors of survival with Alzheimer's disease: a community-based study. Psychol Med. 1995;25(1):171–7. doi:10.1017/S0033291700028191. PMID 7792352.
- ↑ 203.0 203.1 Ganguli M, Dodge HH, Shen C, Pandav RS, DeKosky ST. Alzheimer disease and mortality: a 15-year epidemiological study. Arch. Neurol.. 2005;62(5):779–84. doi:10.1001/archneur.62.5.779. PMID 15883266.
- ↑ 204.0 204.1 204.2 Bermejo-Pareja F, Benito-León J, Vega S, Medrano MJ, Román GC. Incidence and subtypes of dementia in three elderly populations of central Spain. J. Neurol. Sci.. 2008;264(1–2):63–72. doi:10.1016/j.jns.2007.07.021. PMID 17727890.
- ↑ 205.0 205.1 205.2 Di Carlo A. Incidence of dementia, Alzheimer's disease, and vascular dementia in Italy. The ILSA Study. J Am Geriatr Soc. 2002;50(1):41–8. doi:10.1046/j.1532-5415.2002.50006.x. PMID 12028245.
- ↑ Andersen K. Gender differences in the incidence of AD and vascular dementia: The EURODEM Studies. EURODEM Incidence Research Group. Neurology. 1999;53(9):1992–7. PMID 10599770.
- ↑ 2000 U.S. estimates:
- ↑ 208.0 208.1 Ferri CP. Global prevalence of dementia: a Delphi consensus study. Lancet. 2005;366(9503):2112–7. doi:10.1016/S0140-6736(05)67889-0. PMID 16360788.
- ↑ World Health Organization (2006). Neurological Disorders: Public Health Challenges. Switzerland: World Health Organization. pp. 204–207. ISBN 978-92-4-156336-9. http://www.who.int/mental_health/neurology/neurodiso/en/index.html.
- ↑ Auguste D.:
- Alzheimer Alois. Über eine eigenartige Erkrankung der Hirnrinde [About a peculiar disease of the cerebral cortex]. Allgemeine Zeitschrift fur Psychiatrie und Psychisch-Gerichtlich Medizin. 1907;64(1–2):146–148. (German).
- Alzheimer Alois. About a peculiar disease of the cerebral cortex. Alzheimer Dis Assoc Disord. 1987;1(1):3–8. PMID 3331112.
- Maurer Ulrike, Maurer Konrad (2003). Alzheimer: the life of a physician and the career of a disease. New York: Columbia University Press. p. 270. ISBN 0-231-11896-1.
- ↑ Berrios G E. Alzheimer's disease: a conceptual history. Int. J. Ger. Psychiatry. 1990;5(6):355–365. doi:10.1002/gps.930050603.
- ↑ Kraepelin Emil, Diefendorf A. Ross (translated by) (2007-01-17). Clinical Psychiatry: A Textbook For Students And Physicians (Reprint). Kessinger Publishing. p. 568. ISBN 1-4325-0833-4.
- ↑ Katzman Robert, Terry Robert D, Bick Katherine L (editors) (1978). Alzheimer's disease: senile dementia and related disorders. New York: Raven Press. p. 595. ISBN 0-89004-225-X.
- ↑ Boller F, Forbes MM. History of dementia and dementia in history: an overview. J. Neurol. Sci.. 1998;158(2):125–33. doi:10.1016/S0022-510X(98)00128-2. PMID 9702682.
- ↑ Amaducci LA, Rocca WA, Schoenberg BS. Origin of the distinction between Alzheimer's disease and senile dementia: how history can clarify nosology. Neurology. 1986;36(11):1497–9. PMID 3531918.
- ↑ Allegri RF. Economic impact of dementia in developing countries: an evaluation of costs of Alzheimer-type dementia in Argentina. Int Psychogeriatr. 2007;19(4):705–18. doi:10.1017/S1041610206003784. PMID 16870037.
- ↑ Suh GH, Knapp M, Kang CJ. The economic costs of dementia in Korea, 2002. Int J Geriatr Psychiatry. 2006;21(8):722–8. doi:10.1002/gps.1552. PMID 16858741.
- ↑ Wimo A, Jonsson L, Winblad B. An estimate of the worldwide prevalence and direct costs of dementia in 2003. Dement Geriatr Cogn Disord. 2006;21(3):175–81. doi:10.1159/000090733. PMID 16401889.
- ↑ 219.0 219.1 219.2 Moore MJ, Zhu CW, Clipp EC. Informal costs of dementia care: estimates from the National Longitudinal Caregiver Study. J Gerontol B Psychol Sci Soc Sci. 2001;56(4):S219–28. doi:10.1093/geronb/56.4.S219. PMID 11445614.
- ↑ Jönsson L. Determinants of costs of care for patients with Alzheimer's disease. Int J Geriatr Psychiatry. 2006;21(5):449–59. doi:10.1002/gps.1489. PMID 16676288.
- ↑ 221.0 221.1 Zhu CW, Sano M. Economic considerations in the management of Alzheimer's disease. Clin Interv Aging. 2006;1(2):143–54. doi:10.2147/ciia.2006.1.2.143. PMID 18044111.
- ↑ Gaugler JE, Kane RL, Kane RA, Newcomer R. Early community-based service utilization and its effects on institutionalization in dementia caregiving. Gerontologist. 2005;45(2):177–85. doi:10.1093/geront/45.2.177. PMID 15799982.
- ↑ Ritchie K, Lovestone S. The dementias. Lancet. 2002;360(9347):1759–66. doi:10.1016/S0140-6736(02)11667-9. PMID 12480441.
- ↑ Brodaty H, Hadzi-Pavlovic D. Psychosocial effects on carers of living with persons with dementia. Aust N Z J Psychiatry. 1990;24(3):351–61. doi:10.3109/00048679009077702. PMID 2241719.
- ↑ Donaldson C, Tarrier N, Burns A. Determinants of carer stress in Alzheimer's disease. Int J Geriatr Psychiatry. 1998;13(4):248–56. doi:10.1002/(SICI)1099-1166(199804)13:4<248::AID-GPS770>3.0.CO;2-0. PMID 9646153.
- ↑ Pusey H, Richards D. A systematic review of the effectiveness of psychosocial interventions for carers of people with dementia. Aging Ment Health. 2001;5(2):107–19. doi:10.1080/13607860120038302. PMID 11511058.
- ↑ Garrard P, Maloney LM, Hodges JR, Patterson K. The effects of very early Alzheimer's disease on the characteristics of writing by a renowned author. Brain. 2005;128(Pt 2):250–60. doi:10.1093/brain/awh341. PMID 15574466.
- ↑ Sherman FT. Did President Reagan have mild cognitive impairment while in office? Living longer with Alzheimer's Disease. Geriatrics. 2004;59(9):11, 15. PMID 15461232.
- ↑ Venneri A, Forbes-Mckay KE, Shanks MF. Impoverishment of spontaneous language and the prediction of Alzheimer's disease. Brain. 2005;128(Pt 4):E27. doi:10.1093/brain/awh419. PMID 15788549.
- ↑ "Hungary legend Puskas dies at 79". BBC News. 2006-11-17. http://news.bbc.co.uk/sport1/hi/football/europe/6155766.stm. Retrieved 2008-01-25.
- ↑ "Prime Ministers in History: Harold Wilson". London: 10 Downing Street. http://www.number10.gov.uk/history-and-tour/prime-ministers-in-history/harold-wilson. Retrieved 2008-08-18.
- ↑ "Mi padre no reconoció al Rey pero notó el cariño". Madrid: El País. 2008. http://www.elpais.com/articulo/espana/padre/reconocio/Rey/noto/carino/elpepiesp/20080718elpepinac_11/Tes. Retrieved 2008-10-01.
- ↑ "Chicago Rita Hayworth Gala". Alzheimer's Association. 2007. http://www.alz.org/galas/Rita/overview.asp. Retrieved 2010-02-03.
- ↑ "Charlton Heston has Alzheimer's symptoms". CNN. 2002-08-09. http://archives.cnn.com/2002/US/08/09/heston.illness/. Retrieved 2008-01-25.
- ↑ Pauli Michelle (2007-12-12). "Pratchett announces he has Alzheimer's". London: Guardian News and Media. http://www.guardian.co.uk/books/2007/dec/12/news.michellepauli1. Retrieved 2008-08-18.
- ↑ "George Fernandes being treated for Alzheimer's by Yoga Guru Ramdev". DNA. 2010-01-19. http://www.dnaindia.com/india/report_george-fernandes-being-treated-for-alzheimer-s-by-yoga-guru-ramdev_1336547. Retrieved 2010-01-19.
- ↑ "Nobel winner Kao coping with fame and Alzheimer's". China Daily. 2009-10-09. http://www.chinadaily.com.cn/hkedition/2009-10/09/content_8768287.htm. Retrieved 2011-02-06.
- ↑ Bayley John (2000). Iris: a memoir of Iris Murdoch. London: Abacus. ISBN 978-0-349-11215-2. OCLC 41960006.
- ↑ Sparks Nicholas (1996). The notebook. Thorndike, Maine: Thorndike Press. p. 268. ISBN 0-7862-0821-X.
- ↑ "Thanmathra". Webindia123.com. http://www.webindia123.com/movie/regional/thanmatra/index.htm. Retrieved 2008-01-24.
- ↑ Ogiwara Hiroshi (2004) (in (Japanese)). Ashita no Kioku. Tōkyō: Kōbunsha. ISBN 978-4-334-92446-1. OCLC 57352130.
- ↑ Munro Alice (2001). Hateship, Friendship, Courtship, Loveship, Marriage: Stories. New York: A.A. Knopf. ISBN 978-0-375-41300-1. OCLC 46929223. The bear came over the mountain.
- ↑ Malcolm and Barbara:
- ↑ Lashuel HA, Hartley DM, Balakhaneh D, Aggarwal A, Teichberg S, Callaway DJE. New class of inhibitors of amyloid-beta fibril formation. Implications for the mechanism of pathogenesis in Alzheimer's disease. J Biol Chem. 2002;277(45):42881–42890. doi:10.1074/jbc.M206593200. PMID 12167652.
- ↑ Dodel r, Neff F, Noelker C, Pul R, Du Y, Bacher M Oertel W.. Intravenous Immunoglobulins as a Treatment for Alzheimer's Disease: Rationale and Current Evidence. Drugs. 2010;70(5):513–528. doi:10.2165/11533070-000000000-00000. PMID 20329802.
- ↑ Vaccination:
- ↑ "Study Evaluating ACC-001 in Mild to Moderate Alzheimers Disease Subjects". Clinical Trial. US National Institutes of Health. 2008-03-11. http://www.clinicaltrials.gov/ct/show/NCT00498602. Retrieved 2008-06-05.
- ↑ "Study Evaluating Safety, Tolerability, and Immunogenicity of ACC-001 in Subjects With Alzheimer's Disease". US National Institutes of Health. http://clinicaltrials.gov/ct2/show/NCT00479557. Retrieved 2008-06-05.
- ↑ "Alzheimer's Disease Vaccine Trial Suspended on Safety Concern". Medpage Today. 2008-04-18. http://www.medpagetoday.com/MeetingCoverage/AAN/tb/9165. Retrieved 2008-06-14.
- ↑ "Bapineuzumab in Patients With Mild to Moderate Alzheimer's Disease/ Apo_e4 non-carriers". Clinical Trial. US National Institutes of Health. 2008-02-29. http://clinicaltrials.gov/ct2/show/NCT00574132. Retrieved 2008-03-23.
- ↑ "Safety, Tolerability and Efficacy Study to Evaluate Subjects With Mild Cognitive Impairment". Clinical Trial. US National Institutes of Health. 2008-03-11. http://clinicaltrials.gov/ct2/show/NCT00422981. Retrieved 2008-03-23.
- ↑ "Study Evaluating the Safety, Tolerability and Efficacy of PBT2 in Patients With Early Alzheimer's Disease". Clinical Trial. US National Institutes of Health. 2008-01-13. http://clinicaltrials.gov/ct2/show/NCT00471211. Retrieved 2008-03-23.
- ↑ Etanercept research:
- ↑ Wischik Claude M, Bentham Peter, Wischik Damon J, Seng Kwang Meng. Tau aggregation inhibitor (TAI) therapy with remberTM arrests disease progression in mild and moderate Alzheimer's disease over 50 weeks. Alzheimer's & Dementia. 2008 [cited 2008-07-30];4(4):T167. doi:10.1016/j.jalz.2008.05.438.
- ↑ Harrington Charles. Methylthioninium chloride (MTC) acts as a Tau aggregation inhibitor (TAI) in a cellular model and reverses Tau pathology in transgenic mouse models of Alzheimer's disease. Alzheimer's & Dementia. 2008;4(4):T120–T121. doi:10.1016/j.jalz.2008.05.259.
- ↑ Doody RS. Effect of dimebon on cognition, activities of daily living, behaviour, and global function in patients with mild-to-moderate Alzheimer's disease: a randomised, double-blind, placebo-controlled study. Lancet. 2008;372(9634):207–15. doi:10.1016/S0140-6736(08)61074-0. PMID 18640457.
- ↑ "Dimebon Disappoints in Phase 3 Trial". Alzforum.org. http://www.alzforum.org/new/detail.asp?id=2387. Retrieved 2011-02-05.
- ↑ Wozniak M, Mee A, Itzhaki R. Herpes simplex virus type 1 DNA is located within Alzheimer's disease amyloid plaques. J Pathol. 2008;217(1):131–138. doi:10.1002/path.2449. PMID 18973185.
- ↑ Meditation effects on cognitive function and cerebral blood flow in subjects with memory loss: a preliminary study. Journal of Alzheimer's Disease. 2010;20(2):517–26. doi:10.3233/JAD-2010-1391. PMID 20164557. (primary source)
- ↑ Clark CM, Schneider JA, Bedell BJ, Beach TG, Bilker WB, Mintun MA, Pontecorvo MJ, Hefti F, Carpenter AP, Flitter ML, Krautkramer MJ, Kung HF, Coleman RE, Doraiswamy PM, Fleisher AS, Sabbagh MN, Sadowsky CH, Reiman PE, Zehntner SP, Skovronsky DM. FDA recommends approval of new compound in Alzheimer's detection. J Am Med Assoc. 2011-01-19;305(3):275–83. doi:10.1001/jama.2010.2008.
This audio file was created from a revision of the "
Alzheimer's disease" article dated 2008-09-12, and does not reflect subsequent edits to the article. (
Audio help)
- Alzheimer's Disease: Unraveling the Mystery. US Department of Health and Human Services, National Institute on Aging, NIH. 2008. http://www.nia.nih.gov/alzheimers/publication/alzheimers-disease-unraveling-mystery.
- Can Alzheimer's Disease Be Prevented?. US Department of Health and Human Services, National Institute on Aging, NIH. 2009. http://www.globalaging.org/health/us/2009/prevented.pdf.
- Caring for a Person with Alzheimer's Disease: Your Easy-to-Use Guide from the National Institute on Aging. US Department of Health and Human Services, National Institute on Aging, NIH. 2009. http://www.nia.nih.gov/alzheimers/publication/caring-person-alzheimers-disease.
- Cummings JL, Frank JC, Cherry D, Kohatsu ND, Kemp B, Hewett L, Mittman B. Guidelines for managing Alzheimer's disease: Part I. Assessment. American Family Physician. 2002;65(11):2263–2272. PMID 12074525.
- Cummings JL, Frank JC, Cherry D, Kohatsu ND, Kemp B, Hewett L, Mittman B. Guidelines for managing Alzheimer's disease: Part II. Treatment. American Family Physician. 2002;65(12):2525–2534. PMID 12086242.
- Russell D, Barston S, White M (2007-12-19). "Alzheimer's Behavior Management: Learn to manage common behavior problems". helpguide.org. http://www.helpguide.org/elder/alzheimers_behavior_problems.htm. Retrieved 2008-02-29.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physiological/physical behavioral
|
|
|
|
|
|
|
Adult personality and behavior
|
|
|
|
|
|
|
|
|
|
Symptoms and uncategorized
|
|
|
|
|
|
|
|
|
|
|
|
| Inflammation |
|
|
Brain/
encephalopathy |
|
|
|
|
|
|
autoimmune ( Multiple sclerosis, Neuromyelitis optica, Schilder's disease) · hereditary ( Adrenoleukodystrophy, Alexander, Canavan, Krabbe, ML, PMD, VWM, MFC, CAMFAK syndrome) · Central pontine myelinolysis · Marchiafava-Bignami disease · Alpers' disease
|
|
|
|
|
|
|
|
|
|
|
Other
|
|
|
|
Spinal cord/
myelopathy |
|
|
| Both/either |
|
|
|
|
|





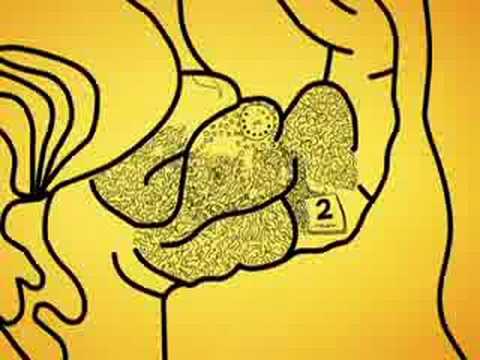



















































")








_Presenile_Onset.Jpg)


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}